Korean Circ J.
2018 Jan;48(1):59-70. 10.4070/kcj.2017.0058.
Association of Syntax Score II with Contrast-induced Nephropathy and Hemodialysis Requirement in Patients with ST Segment Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention
- Rencuzogullari I

- Çağdaş
- Karakoyun
- KarabaÄŸ Y
- Yesin M
- Gürsoy MO
- Artaç I
- Ä°liÅŸ D
- Efe SC
- Tural K
- TanboÄŸa I
- Affiliations
-
- 1Department of Cardiology, Kafkas University Medical Faculty, Kars, Turkey. rencuzog@gmail.com
- 2Department of Cardiology, Kars Harakani State Hospital, Kars, Turkey.
- 3Department of Cardiology, Gaziemir State Hospital, Ä°zmir, Turkey.
- 4Department of Cardiology, Ağrı State Hospital, Ağrı, Turkey.
- 5Department of Cardiovascular Surgery, Kafkas University Medical Faculty, Kars, Turkey.
- 6Department of Cardiology, Ataturk University Medical Faculty, Erzurum, Turkey.
- KMID: 2405046
- DOI: http://doi.org/10.4070/kcj.2017.0058
Abstract
- BACKGROUND AND OBJECTIVES
Contrast-induced nephropathy (CIN) is a common complication of primary percutaneous coronary intervention (pPCI) and is associated with high mortality and morbidity and long hospital stay in patients with ST elevation myocardial infarction (STEMI). The Syntax Score (SS) has previously been studied in STEMI patients, and it was associated with increased CIN development and long-term mortality. This study investigates a possible relationship between CIN development and Syntax Score II (SSII) and compares SS and SSII by assessing CIN risk in STEMI patients treated with pPCI.
METHODS
A total of 1,234 patients who underwent pPCI were divided into 2 groups according to CIN development. Patients with CIN were further divided into 2 groups according to whether or not they required hemodialysis. Reclassification tables, net reclassification improvement, and integrated discriminative improvement methods were used to assess the additive predictive value of SSII for predicting CIN.
RESULTS
In the present study, 166 patients (13.5%) had CIN. Although both SS and SSII were significantly higher in CIN patients, only SSII was an independent predictor of CIN (odds ratio [OR], 1.031; 95% confidence interval [CI], 1.012-1.051; p < 0.001) and hemodialysis requirement (OR, 1.078; 95% CI, 1.046-1.078; p < 0.001). When comparing SSII and SS in their ability to determine CIN risk, we found SSII to have a reclassification improvement of 27.59% (p < 0.001) and an integrated discrimination improvement of 9.1% (p < 0.001).
CONCLUSIONS
The combination of clinical and anatomic variables can more accurately identify patients who are at high risk for CIN after pPCI. While SSII is harder to calculate than SS, it provides better prediction for CIN and hemodialysis requirement than SS.
MeSH Terms
Figure
-

Figure 1 Survival curve comparison between patients with and without CIN during hospitalization. CIN = contrast-induced nephropathy.
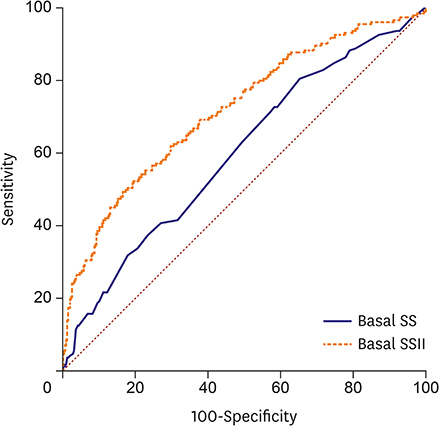
Figure 2 ROC graphics to detect cutoff values of SS and SSII for CIN prediction. CIN = contrast-induced nephropathy; ROC = receiver operating characteristics; SS = Syntax Score; SSII = Syntax Score II.
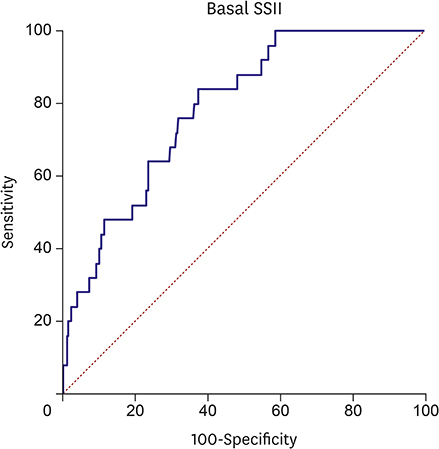
Figure 3 ROC graphics to detect cutoff values of SSII for hemodialysis requirement. ROC = receiver operating characteristics; SSII = Syntax Score II.
Cited by 1 articles
-
Contrast-induced Acute Kidney Injury and Inflammation
Kyeong Ho Yun
Korean Circ J. 2018;48(1):84-85. doi: 10.4070/kcj.2017.0357.
Reference
-
1. Xhepa E, Tada T, Kufner S, et al. Long-term prognostic value of risk scores after drug-eluting stent implantation for unprotected left main coronary artery: a pooled analysis of the ISAR-LEFT-MAIN and ISAR-LEFT-MAIN 2 randomized clinical trials. Catheter Cardiovasc Interv. 2017; 89:1–10.
Article2. Gupta R, Gurm HS, Bhatt DL, Chew DP, Ellis SG. Renal failure after percutaneous coronary intervention is associated with high mortality. Catheter Cardiovasc Interv. 2005; 64:442–448.
Article3. Liss P, Persson PB, Hansell P, Lagerqvist B. Renal failure in 57 925 patients undergoing coronary procedures using iso-osmolar or low-osmolar contrast media. Kidney Int. 2006; 70:1811–1817.4. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004; 44:1393–1399.5. McCullough PA. Contrast-induced acute kidney injury. J Am Coll Cardiol. 2008; 51:1419–1428.
Article6. McCullough PA, Wolyn R, Rocher LL, Levin RN, O'Neill WW. Acute renal failure after coronary intervention: incidence, risk factors, and relationship to mortality. Am J Med. 1997; 103:368–375.7. Oduncu V, Erkol A, Karabay CY, et al. Relation of the severity of contrast induced nephropathy to SYNTAX score and long term prognosis in patients treated with primary percutaneous coronary intervention. Int J Cardiol. 2013; 168:3480–3485.
Article8. Elbasan Z, Şahin DY, Gür M, et al. Contrast-induced nephropathy in patients with ST elevation myocardial infarction treated with primary percutaneous coronary intervention. Angiology. 2014; 65:37–42.
Article9. Wang G, Wang C, Zhang Y, et al. Usefulness of the SYNTAX score II to predict 1-year outcome in patients with primary percutaneous coronary intervention. Coron Artery Dis. 2016; 27:483–489.
Article10. Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC). Steg PG, James SK, et al. ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012; 33:2569–2619.11. Thomsen HS. Guidelines for contrast media from the European Society of Urogenital Radiology. AJR Am J Roentgenol. 2003; 181:1463–1471.
Article12. Kim SM, Tripathy DR, Park SW, et al. Impact of chronic kidney disease on clinical outcomes in diabetic patients undergoing percutaneous coronary intervention in the era of newer-generation drug-eluting stents. Korean Circ J. 2017; 47:222–230.
Article13. SYNTAX Working Group. SYNTAX score calculator [Internet]. [place unknown]: SYNTAX Working Group;cited 2016 September 25. Available from: http://www.syntaxscore.com.14. Sianos G, Morel MA, Kappetein AP, et al. The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention. 2005; 1:219–227.15. Magro M, Nauta S, Simsek C, et al. Value of the SYNTAX score in patients treated by primary percutaneous coronary intervention for acute ST-elevation myocardial infarction: the MI SYNTAX score study. Am Heart J. 2011; 161:771–781.16. Farooq V, van Klaveren D, Steyerberg EW, et al. Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients: development and validation of SYNTAX score II. Lancet. 2013; 381:639–650.
Article17. Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation. 1996; 93:879–888.18. Youden WJ. Index for rating diagnostic tests. Cancer. 1950; 3:32–35.
Article19. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988; 44:837–845.
Article20. Pencina MJ, D'Agostino RB Sr, D'Agostino RB Jr, Vasan RS. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med. 2008; 27:157–172.
Article21. Tziakas D, Chalikias G, Stakos D, et al. Development of an easily applicable risk score model for contrast-induced nephropathy prediction after percutaneous coronary intervention: a novel approach tailored to current practice. Int J Cardiol. 2013; 163:46–55.22. Rihal CS, Textor SC, Grill DE, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002; 105:2259–2264.
Article23. Dangas G, Iakovou I, Nikolsky E, et al. Contrast-induced nephropathy after percutaneous coronary interventions in relation to chronic kidney disease and hemodynamic variables. Am J Cardiol. 2005; 95:13–19.
Article24. Harjai KJ, Raizada A, Shenoy C, et al. A comparison of contemporary definitions of contrast nephropathy in patients undergoing percutaneous coronary intervention and a proposal for a novel nephropathy grading system. Am J Cardiol. 2008; 101:812–819.
Article25. Subramaniam RM, Suarez-Cuervo C, Wilson RF, et al. Effectiveness of prevention strategies for contrast-induced nephropathy: a systematic review and meta-analysis. Ann Intern Med. 2016; 164:406–416.26. John S, Schmieder RE. Potential mechanisms of impaired endothelial function in arterial hypertension and hypercholesterolemia. Curr Hypertens Rep. 2003; 5:199–207.
Article27. Aykan AÇ, Gül I, Gökdeniz T, et al. Is coronary artery disease complexity valuable in the prediction of contrast induced nephropathy besides Mehran risk score, in patients with ST elevation myocardial infarction treated with primary percutaneous coronary intervention? Heart Lung Circ. 2013; 22:836–843.
Article28. Fu NK, Yang SC, Chen YL, et al. Risk factors and scoring system in the prediction of contrast induced nephropathy in patients undergoing percutaneous coronary intervention. Zhonghua Yi Xue Za Zhi. 2012; 92:551–554.29. Vuruşkan E, Saraçoğlu E. Bilirubin levels are associated with contrast-induced nephropathy in peripheral artery disease. Angiology. 2017; 68:728–733.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current Status of Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction and Multivessel Coronary Artery Disease
- Missing Right Coronary Artery in a Patient with Acute Inferior ST Segment Elevation Myocardial Infarction: A Case of Extremely Rare Variation of Coronary Anatomy
- A Case of Coronary Artery Dissection after Blunt Chest Trauma Resulting in ST-Segment Elevation Myocardial Infarction
- The Operator Volume of Primary Percutaneous Coronary Intervention for ST Segment Elevation Myocardial Infarction Does Not Guarantee Its Quality in Korea
- Consecutive Multivessel Myocardial Infarction during Primary Percutaneous Coronary Intervention
