Infectious Pseudoaneurysm Caused by Group A Streptococcus in a Child without Underlying Disease
- Affiliations
-
- 1Department of Pediatrics, Kosin University Gospel Hospital, Kosin University College of Medicine, Busan, the Republic of Korea. shine707@hanmail.net
- 2Department of Pediatrics, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, the Republic of Korea.
- KMID: 2401394
- DOI: http://doi.org/10.14776/piv.2017.24.3.183
Abstract
- Group A streptococcus is a common cause of upper respiratory infection in children; however, it is a rare cause of pseudoaneurysm in pediatrics with only limited reports of cases associated with cardiac surgery and underlying disease. We report a case of infectious pseudoaneurysm of the right internal iliac artery caused by group A streptococcus in a previously healthy 5-year-old boy who presented with scarlet fever and group A streptococcal bacteremia. He was admitted to the hospital with fever, rash on the whole body, and sore throat, accompanied by severe leg pain. He was treated with surgical removal and antibiotics. Because a pseudoaneurysm may develop in children without vascularrelated underlying diseases, we should consider the possibility of this important clinical diagnosis in patients with scarlet fever.
MeSH Terms
Figure
-
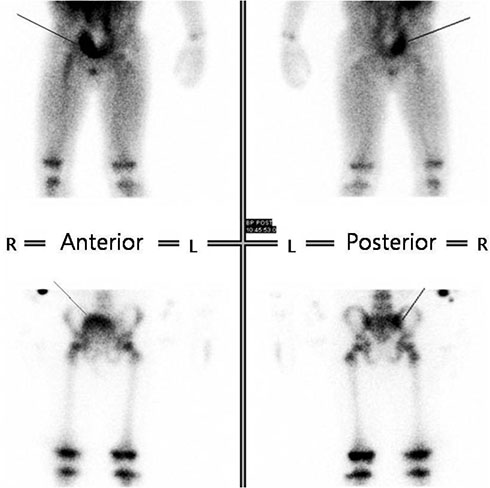
Figure 1 Bone scan. There are increased perfusion and blood pool activity on right sacroiliac joint (solid lines).
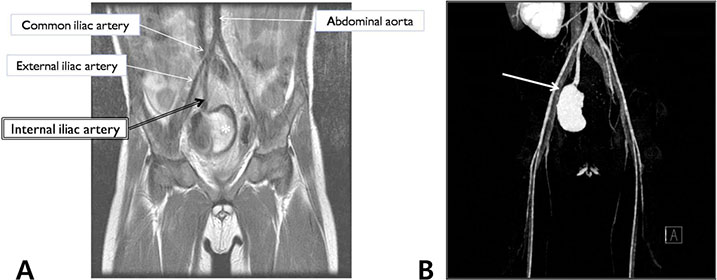
Figure 2 (A) Magnetic resonance imaging of lower extremities. Fusiform signal void with heterogeneously high signal lesion (asterisk) seems to be arising from right internal iliac artery. (B) Computed tomography angiography of lower extremities. There is a large pseudoaneurysm in pelvic cavity, which originates from the anterior branch of right internal iliac artery (arrow).
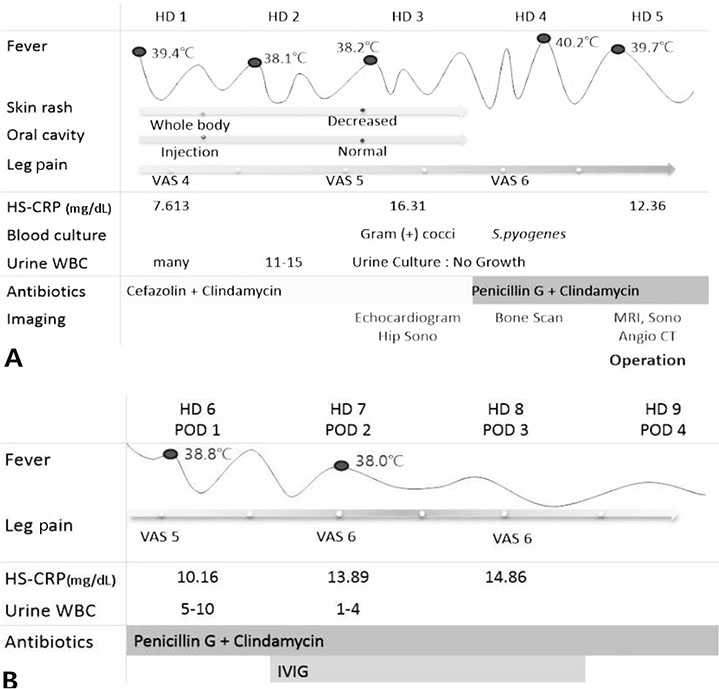
Figure 3 (A) The clinical course before the operation. (B) The clinical course after the operation. Abbreviations: HD, hospital day; VAS, visual analogue scale for pain; HS-CRP, high-sensitivity C-reactive protein; WBC, white blood cell; Sono, ultrasonography; MRI, magnetic resonance imaging; Angio CT, computed tomography angiography; POD, postoperative day; IVIG, intravenous immunoglobulin; S. pyogenes, Streprococcus pyogenes.
Reference
-
1. Shulman ST. Group A Streptococcus. Kliegman RM, Stanton BM, Geme J, Schor NF, editors. Nelson textbook of pediatrics. 20th ed. Philadelphia: Elsevier Inc.;2016. p. 1327–1337.2. World Health Organization. The current evidence for the burden of Group A Streptococcal diseases [Internet]. Geneva: WHO;c2017. cited 2017 Nov 18. Available from: http://www.who.int/maternal_child_adolescent/documents/fch_cah_05_07/en/.3. Lee HJ. Multicenetric approach for analysis of serotypes of pneumococcus isolated from invasive infections in Korean children (3rd year) [Internet]. Seoul: Korea Centers for Disease Control and Prevention;2013. cited 2017 Nov 18. Available from: http://cdc.go.kr/CDC/cms/cmsFileDownload.jsp?fid=28&cid=61767&fieldName=attach1&index=1.4. Korea Centers for Disease Control and Prevention. Infectious diseases surveillance yearbook, 2014 [Internet]. Cheongju: Korea Centers for Disease Control and Prevention;2015. cited 2017 Nov 18. Available from: http://cdc.go.kr/CDC/cms/content/mobile/86/69386_view.html.5. Barth H, Moosdorf R, Bauer J, Schranz D, Akinturk H. Mycotic pseudoaneurysm of the aorta in children. Pediatr Cardiol. 2000; 21:263–266.
Article6. Biswas JS, Lyons OT, Bell RE, Price N. Extra-aortic mycotic aneurysm due to group A Streptococcus after pharyngitis. J Clin Microbiol. 2013; 51:2797–2799.
Article7. Bergsland J, Kawaguchi A, Roland JM, Pieroni DR, Subramanian S. Mycotic aortic aneurysms in children. Ann Thorac Surg. 1984; 37:314–318.
Article8. Restrepo MS, Turek JW, Reinking B, Bergen NV. Mycotic aneurysm in a child with history of coarctation of the aorta repair. Ann Pediatr Cardiol. 2014; 7:138–141.
Article9. Sarkar R, Coran AG, Cilley RE, Lindenauer SM, Stanley JC. Arterial aneurysms in children: clinicopathologic classification. J Vasc Surg. 1991; 13:47–56.
Article10. Millar AJ, Gilbert RD, Brown RA, Immelman EJ, Burkimsher DA, Cywes S. Abdominal aortic aneurysms in children. J Pediatr Surg. 1996; 31:1624–1628.
Article11. Chantepie A, Robert M, Pelletier J, Gold F, Mercier C, Lacombe A, et al. Mycotic aneurysm of bronchial artery. Apropos of a case in an infant. Chir Pediatr. 1980; 21:407–410.12. Tachibana K, Takagi N, Kannki K, Higami T. Mycotic aneurysm of ascending aorta in an infant. Asian Cardiovasc Thorac Ann. 2013; 21:79–81.
Article13. Hoffman MA, Ramey AK, Hammel J, Truemper E, Kutty S, Chatterjee A. Recurrent mycotic aneurysm in a 2-yearold boy with group A Streptococcus bacteremia. Pediatr Infect Dis J. 2012; 31:1080–1082.
Article14. Kim YW. Infected aneurysm: current management. Ann Vasc Dis. 2010; 3:7–15.
Article15. Ferretti JJ, Stevens DL, Fischetti VA. Streptococcus pyogenes: basic biology to clinical manifestations [Internet]. Oklahoma City: The University of Oklahoma Health Sciences Center;2016. cited 2017 Nov 18. Available from: https://www.ncbi.nlm.nih.gov/books/NBK333424/pdf/Bookshelf_NBK333424.pdf.16. Kaul R, McGeer A, Norrby-Teglund A, Kotb M, Schwartz B, O'Rourke K, et al. Intravenous immunoglobulin therapy for streptococcal toxic shock syndrome: a comparative observational study. The Canadian Streptococcal Study Group. Clin Infect Dis. 1999; 28:800–807.
Article17. Carapetis JR, Jacoby P, Carville K, Ang SJ, Curtis N, Andrews R. Effectiveness of clindamycin and intravenous immunoglobulin, and risk of disease in contacts, in invasive group a streptococcal infections. Clin Infect Dis. 2014; 59:358–365.
Article18. Shah SS, Hall M, Srivastava R, Subramony A, Levin JE. Intravenous immunoglobulin in children with streptococcal toxic shock syndrome. Clin Infect Dis. 2009; 49:1369–1376.
Article19. Ogawa T, Terao Y, Sakata H, Okuni H, Ninomiya K, Ikebe K, et al. Epidemiological characterization of Streptococcus pyogenes isolated from patients with multiple onsets of pharyngitis. FEMS Microbiol Lett. 2011; 318:143–151.
Article20. Rasmussen M. Recurrent sepsis caused by Streptococcus pyogenes. J Clin Microbiol. 2011; 49:1671–1673.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Septic Knee Arthritis Caused by Streptococcus sanguis in a Patient with Osteoarthritis of the Knee
- Streptococcus Spondylitis Concomitant Infectious Endocarditis: A Case Report
- A Case of Pseudoaneurysm of the Superior Thyroid Artery after Core Needle Biopsy
- Two Cases of Liver Abscess Caused by Group G beta-Hemolytic Streptococcus
- Gas Gangrene Caused by Streptococcus anginosus
