Rapid Progression of Bilateral Vestibulopathy Due to Metastatic Lung Cancer
- Affiliations
-
- 1Department of Neurology, Kyungpook National University School of Medicine, Daegu, Korea.
- 2Research Administration Team, Seoul National University Bundang Hospital, Seongnam, Korea.
- 3Department of Neurology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. jisookim@snu.ac.kr
- KMID: 2399608
- DOI: http://doi.org/10.3988/jcn.2018.14.1.104
Abstract
- No abstract available.
MeSH Terms
Figure
-
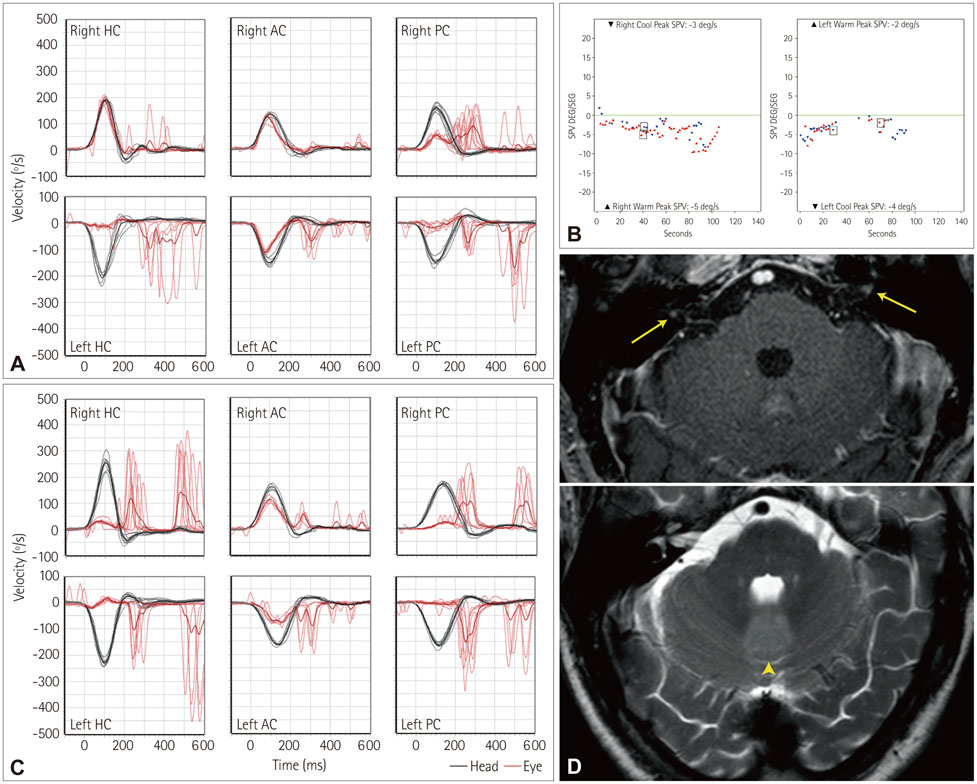
Fig. 1 A: The vestibulo-ocular reflex (VOR) gain values are decreased for left horizontal (HC, 0.1, normal range ≥0.8) and both posterior canals (PCs, 0.3 for the right PC, and 0.1 for the left PC, normal range ≥0.7), but normal for right horizontal and both anterior canals (ACs, 1.0 for the right HC, 0.9 for the right AC, and 0.8 for the left AC, normal range ≥0.7). Overt saccades are found for these canals with decreased VOR gains, while covert saccades are observed during stimulation of the right PC and left AC. B: Caloric tests show bilaterally reduced responses with the summated slow phase velocities (SPVs) of the induced nystagmus at 14°/s (8°/s in the right ear, 6°/s in the left ear). C: Video head impulse tests one week later document reduced VOR gains and overt catch-cup saccades for all six semicircular canals (0.2 for the right HC, 0.1 for the left HC, 0.6 for the right AC, 0.4 for the left AC, 0.1 for the right PC, 0.0 for the left PC). D: Brain MRIs reveals nodular gadolinium enhancements within both internal auditory canals (arrows) in addition to increased signals in the cerebellar vermis (arrowheads). ACs: anterior canals, HC: horizontal canal, PCs: posterior canals, SPV: slow phase velocity, VOR: vestibulo-ocular reflex.
Reference
-
1. Choi SY, Kee HJ, Park JH, Kim HJ, Kim JS. Combined peripheral and central vestibulopathy. J Vestib Res. 2014; 24:443–451.
Article2. Lucieer F, Vonk P, Guinand N, Stokroos R, Kingma H, van de. Bilateral vestibular hypofunction: insights in etiologies, clinical subtypes, and diagnostics. Front Neurol. 2016; 7:26.
Article3. Krainik A, Cyna-Gorse F, Bouccara D, Cazals-Hatem D, Vilgrain V, Denys A, et al. MRI of unusual lesions in the internal auditory canal. Neuroradiology. 2001; 43:52–57.
Article4. Chang MT, Michaelides EM. High rate of bilaterality in internal auditory canal metastases. Am J Otolaryngol. 2015; 36:798–804.
Article5. Yuh WT, Mayr-Yuh NA, Koci TM, Simon JH, Nelson KL, Zyroff J, et al. Metastatic lesions involving the cerebellopontine angle. Am J Neuroradiol. 1993; 14:99–106.6. Weber KP, Aw ST, Todd MJ, McGarvie LA, Curthoys IS, Halmagyi GM. Horizontal head impulse test detects gentamicin vestibulotoxicity. Neurology. 2009; 72:1417–1424.
Article7. Zingler VC, Weintz E, Jahn K, Mike A, Huppert D, Rettinger N, et al. Follow-up of vestibular function in bilateral vestibulopathy. J Neurol Neurosurg Psychiatry. 2008; 79:284–288.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bilateral Vestibular Hypofunction Induced by Unilateral Herpes Zoster Oticus
- A Suspected Case of Metastatic Tumors Involving Both Internal Auditory Canals
- A Case of Bilateral Semicircular Canal Dysplasia with Normal Cochlear Found in Bilateral Vestibulopathy
- Acute Bilateral Vestibulopathy with Concomitant Progressive Deterioration of Binaural Hearing
- A Case of Bilateral Vestibulopathy Caused by Varicella-Zoster Meningitis
