Childhood allergic bronchopulmonary aspergillosis presenting as a middle lobe syndrome
- Affiliations
-
- 1Department of Pulmonary Medicine, Vallabhbhai Patel Chest Institute, University of Delhi, Delhi 110 007, India. ashokshah99@yahoo.com
- KMID: 2396972
- DOI: http://doi.org/10.5415/apallergy.2016.6.1.67
Abstract
- Allergic bronchopulmonary aspergillosis (ABPA) is infrequently documented in children with asthma. Although collapse is not uncommon, middle lobe syndrome (MLS) as a presentation of ABPA is rather a rarity. A 9-year-old female child with asthma presented with increase in intensity of symptoms along with a right midzone patchy consolidation on a chest radiograph. In addition, an ill-defined opacity abutting the right cardiac border with loss of cardiac silhouette was noted. A right lateral view confirmed a MLS, which was further corroborated by high resolution computed tomography. Central bronchiectasis was also observed, which prompted a work-up for ABPA. The child met 7/8 major diagnostic criteria for ABPA. She was then initiated on oral prednisolone that resulted in a marked clinical improvement within a fortnight. Radiological clearance occurred at 3 months with inflation of the middle lobe. ABPA presenting with MLS in a child is yet to be reported. A high index of suspicion is required to establish the diagnosis of ABPA in a child presenting with MLS. This would obviate the invasive investigations usually done to ascertain the cause of MLS.
Keyword
MeSH Terms
Figure
-
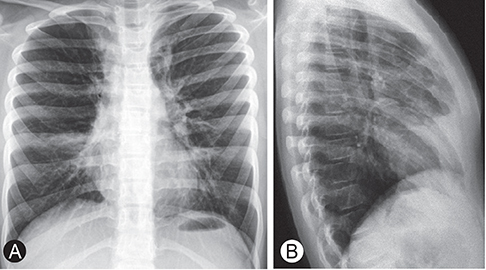
Fig. 1 (A) Chest radiograph posteroanterior view showing a right midzone patchy consolidation and an ill-defined opacity abutting the right cardiac border with loss of cardiac silhouette. (B) Chest radiograph right lateral view showing a wedge shaped density extending from the hilum anteriorly and inferiorly along with loss of volume confirming a middle lobe syndrome.

Fig. 2 (A) High resolution computed tomography (HRCT) (mediastinal window) of the thorax showing middle lobe syndrome. (B) HRCT (lung window) of the thorax showing central bronchiectasis.
Cited by 2 articles
-
Asia Pacific Allergy: it's been five years!
Yoon-Seok Chang
Asia Pac Allergy. 2016;6(1):1-2. doi: 10.5415/apallergy.2016.6.1.1.A review of 42 asthmatic children with allergic bronchopulmonary aspergillosis
Ashok Shah, Shekhar Kunal
Asia Pac Allergy. 2017;7(3):148-155. doi: 10.5415/apallergy.2017.7.3.148.
Reference
-
1. Shah A, Panjabi C. Allergic aspergillosis of the respiratory tract. Eur Respir Rev. 2014; 23:8–29.
Article2. Shah A, Kala J, Sahay S. Allergic bronchopulmonary aspergillosis with hilar adenopathy in a 42-month-old boy. Pediatr Pulmonol. 2007; 42:747–748.
Article3. Imbeau SA, Cohen M, Reed CE. Allergic bronchopulmonary aspergillosis in infants. Am J Dis Child. 1977; 131:1127–1130.
Article4. Graham EA, Burford TH, Mayer JH. Middle lobe syndrome. Postgrad Med. 1948; 4:29–34.
Article5. Brock RC, Cann RJ, Dickinson JR. Tuberculous mediastinal lymphadenitis in childhood: secondary effects on the lungs. Guys Hosp Rep. 1937; 87:295–317.6. Eisenberg RS, Valdesuso C. Middle lobe syndrome secondary to allergic bronchopulmonary aspergillosis. Ann Allergy. 1980; 44:217–219.7. Shah A, Bhagat R, Panchal N, Jaggi OP, Khan ZU. Allergic bronchopulmonary aspergillosis with middle lobe syndrome and allergic Aspergillus sinusitis. Eur Respir J. 1993; 6:917–918.8. Shah A, Behera S, Panjabi C. Middle lobe syndrome: a rare presentation of allergic bronchopulmonary aspergillosis. Eur Ann Allergy Clin Immunol. 2014; 46:147–151.9. Rosenberg M, Patterson R, Mintzer R, Cooper BJ, Roberts M, Harris KE. Clinical and immunologic criteria for the diagnosis of allergic bronchopulmonary aspergillosis. Ann Intern Med. 1977; 86:405–414.
Article10. Wang JL, Patterson R, Rosenberg M, Roberts M, Cooper BJ. Serum IgE and IgG antibody activity against Aspergillus fumigatus as a diagnostic aid in allergic bronchopulmonary aspergillosis. Am Rev Respir Dis. 1978; 117:917–927.11. Gudbjartsson T, Gudmundsson G. Middle lobe syndrome: a review of clinicopathological features, diagnosis and treatment. Respiration. 2012; 84:80–86.
Article12. Romagnoli V, Priftis KN, de Benedictis FM. Middle lobe syndrome in children today. Paediatr Respir Rev. 2014; 15:188–193.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Allergic Bronchopulmonary Aspergillosis Forming Broncholith Misdiagnosed as an Uncontrolled Asthma with Broncholithiasis
- Diagnosis and Treatment of Allergic Bronchopulmonary Aspergillosis
- A Case of Endobronchial Aspergillosis Completely Obstructing Lobar Bronchus
- Asymptomatic Developments of Pulmonary Infiltrates and Central Bronchiectasis in a Patient with Allergic Bronchopulmonary Aspergillosis
- Pulmonary Aspergillosis
