Non-Calcified Ductal Carcinoma in Situ: Ultrasound and Mammographic Findings Correlated with Histological Findings
- Affiliations
-
- 1Department of Radiology, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea. seoboky@korea.ac.kr
- 2Department of Radiology, Korea University Ansan Hospital, Korea University College of Medicine, Ansan-city, Gyeonggi-do, Korea.
- 3Department of Radiology, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea.
- 4Department of Radiology, Korea University Guro Hospital, Korea University College of Medicine, Seoul, Korea.
Abstract
- PURPOSE
To evaluate radiological findings of non-calcified ductal carcinoma in situ (DCIS) and to correlate those with histological features. MATERIALS AND METHODS: From July 2002 to March 2006, 22 patients with histologically-proven non-calcified DCIS were included. Mammography was obtained in 19 patients, ultrasound in 18 patients, and both examinations in 15 patients. Radiological findings were evaluated according to the Breast Imaging Reporting and Data System by American College of Radiology. Histological tumor subtype and Van Nuys classification of DCIS were assessed. RESULTS: Histological subtypes consisted of mixed type in 11 patients (50%), comedo in 4 (18%), cribriform in 4 (18%), papillary type in 2 (9%), and solid in one (5%). According to Van Nuys classification, group 3 DCIS was observed in 13 (59%) patients. In the 19 patients who underwent mammography, 13 patients presented with abnormal findings: focal asymmetry in 7 patients (37%), masses in 4 (21%), skin thickening in one (5%), and architectural distortion in one (5%). In the 18 patients who had received breast ultrasound, a mass was present in 15 (83%) patients and ductal changes in 3 patients (17%). Sixty percent of patients with masses on ultrasound had group 3 DCIS and 100% of patients with ductal change had group 1 DCIS (p=0.017). CONCLUSION: Diagnosis of non-calcified DCIS by mammography is not an easy task due to the lack of typical malignant calcifications or masses. High resolution ultrasound can be useful for detecting non-calcified DCIS, and ultrasound findings are correlated with histological features.
Keyword
MeSH Terms
Figure
-
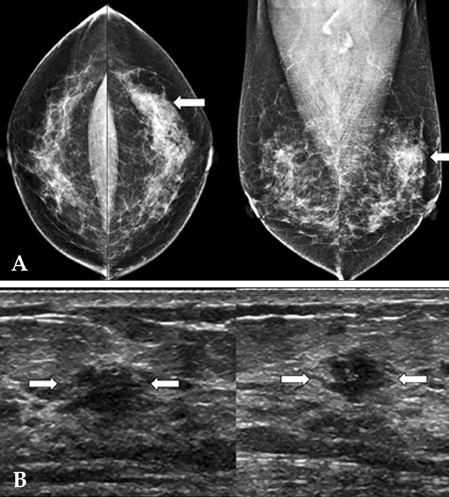
Fig. 1 (Patient No. 5) A 35-year-old woman with a palpable mass in left breast and group 3 DCIS of Van Nuys classification (A) Mammography shows a focal asymmetry (arrows) in the left upper outer quadrant, palpable mass site. (B) Transverse (left) and longitudinal (right) scans of US reveal a microlobulated marginated, irregular shaped, hypoechoic mass (arrows). The mass has parallel orientation and an unaffected posterior acoustic feature.
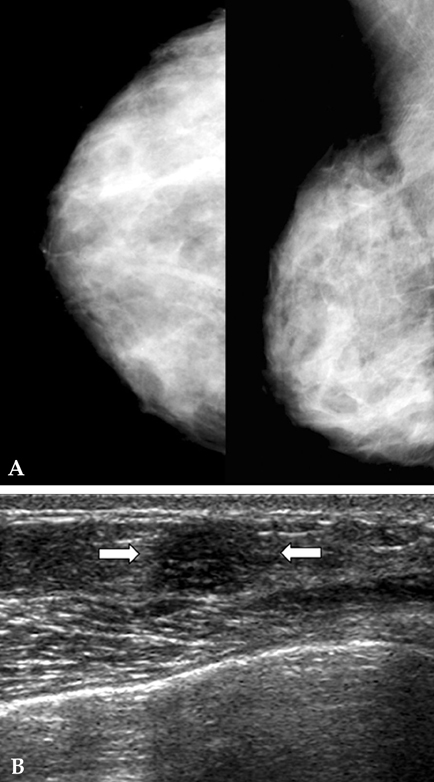
Fig. 2 (Patient No. 8) A 42 -year-old woman with a palpable mass in the right breast and group 3 DCIS of Van Nuys classification. (A) Right mammography shows no detectable lesion. (B) Transverse scan of US demonstrates an indistinct marginated, oval shaped, hypoechoic mass (arrows) in the lower mid portion of right breast, palpable mass site. The mass has parallel orientation and an unaffected posterior acoustic feature.

Fig. 3 (Patient No. 12) A 45-year-old woman with left bloody discharge and group 1 DCIS of Van Nuys classification. (A) Mammography shows no detectable abnormal finding. (B) Transverse scan of US depicts ductectasia with intraductal solid components (arrows) in the central portion of the left breast.
Reference
-
1. Dershaw DD, Abramson A, Kinne DW. Ductal carcinoma in situ: mammographic findings and clinical implications. Radiology. 1989. 170:411–415.
Article2. Holland R, Hendriks JH, Vebeek AL, Mravunac M, Schuurmans Stekhoven JH. Extent, distribution, and mammographic/histological correlations of breast ductal carcinoma in situ. Lancet. 1990. 335:519–522.
Article3. Schnitt SJ, Silen W, Sadowsky NL, Connolly JL, Harris JR. Ductal carcinoma in situ (intraductal carcinoma) of the breast. N Engl J Med. 1988. 318:898–903.
Article4. Stomper PC, Connolly JL. Ductal carcinoma in situ of the breast: correlation between mammographic calcification and tumor subtype. AJR Am J Roentgenol. 1992. 159:483–485.
Article5. Ernster VL, Barclay J, Kerlikowske K, Wilkie H, Ballard-Barbash R. Mortality among women with ductal carcinoma in situ of the breast in the population-based surveillance, epidemiology and end results program. Arch Intern Med. 2000. 160:953–958.
Article6. Ikeda DM, Andersson I. Ductal carcinoma in situ: atypical mammographic appearances. Radiology. 1989. 172:661–666.
Article7. Stomper PC, Connolly JL, Meyer JE, Harris JR. Clinically occult ductal carcinoma in situ detected with mammography: analysis of 100 cases with radiologic-pathologic correlation. Radiology. 1989. 172:235–241.
Article8. Holland R, Peterse JL, Millis RR, Eusebi V, Faverly D, van de Vijver MJ, et al. Ductal carcinoma in situ: a proposal for a new classification. Semin Diagn Pathol. 1994. 11:167–180.9. Berg WA, Gilbreath PL. Multicentric and multifocal cancer: whole-breast US in preoperative evaluation. Radiology. 2000. 214:59–66.
Article10. Crystal P, Strano SD, Shcharynski S, Koretz MJ. Using sonography to screen women with mammographically dense breasts. AJR Am J Roentgenol. 2003. 181:177–182.
Article11. Kaplan SS. Clinical utility of bilateral whole-breast US in the evaluation of women with dense breast tissue. Radiology. 2001. 221:641–649.
Article12. Leconte I, Feger C, Galant C, Berlière M, Berg BV, D'Hoore W, et al. Mammography and subsequent whole-breast sonography of nonpalpable breast cancers: the importance of radiologic breast density. AJR Am J Roentgenol. 2003. 180:1675–1679.
Article13. Stavros AT, Thickman D, Rapp CL, Dennis MA, Parker SH, Sisney GA. Solid breast nodules: use of sonography to distinguish between benign and malignant lesions. Radiology. 1995. 196:123–134.
Article14. DiPiro PJ, Meyer JE, Denison CM, Frenna TH, Harvey SC, Smith DN. Image-guided core breast biopsy of ductal carcinoma in situ presenting as a non-calcified abnormality. Eur J Radiol. 1999. 30:231–236.
Article15. Moon WK, Myung JS, Lee YJ, Park IA, Noh DY, Im JG. US of ductal carcinoma in situ. Radiographics. 2002. 22:269–280. discussion 80-81.
Article16. American College of Radiology. BI-RADS Committee. ACR BI-RADS® breast imaging and reporting data system: breast imaging atlas. 2003. Reston, VA: American College of Radiology.17. Consensus Conference Committee. Consensus conference on the classification of ductal carcinoma in situ. Hum Pathol. 1997. 28:1221–1225.18. Poller DN, Silverstein MJ, Galea M, Locker AP, Elston CW, Blamey RW, et al. Ideas in pathology. Ductal carcinoma in situ of the breast: a proposal for a new simplified histological classification association between cellular proliferation and c-erbB-2 protein expression. Mod Pathol. 1994. 7:257–262.19. Silverstein MJ, Poller DN, Waisman JR, Colburn WJ, Barth A, Gierson ED, et al. Prognostic classification of breast ductal carcinoma-in-situ. Lancet. 1995. 345:1154–1157.
Article20. Holland R, Hendriks JH. Microcalcifications associated with ductal carcinoma in situ: mammographic-pathologic correlation. Semin Diagn Pathol. 1994. 11:181–192.21. Yang WT, Tse GM. Sonographic, mammographic, and histopathologic correlation of symptomatic ductal carcinoma in situ. AJR Am J Roentgenol. 2004. 182:101–110.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis of Ductal Carcinoma in situ: Role of Additional Breast Sonography
- Analysis of X-ray Mammographic Findings of Breast Carcinoma according to Histopathologic Classification
- Ductal Carcinoma in Situ: US Finding and Its Usefulness
- Predictive Factors of Residual Invasive Breast Cancer after Core Biopsy for Ductal Carcinoma in Situ
- Comparative Analysis Among X-ray Mammographic Findings, Nuclear and Histologic Grading, and TNM Staging of Breast Carcinoma
