Complete Reversal of Diffusion Restriction after Treatment of Traumatic Carotid-Cavernous Fistula
- Affiliations
-
- 1Department of Neurosurgery, Shim Jeong Hospital, Seoul, Korea.
- 2Department of Neurosurgery, CHA Bundang Medical Center, CHA University, Seongnam, Korea. hanib@cha.ac.kr
- KMID: 2394556
- DOI: http://doi.org/10.13004/kjnt.2017.13.2.171
Abstract
- A 15-year-old man presented with stupor following a motorcycle traffic accident. The patient was diagnosed with a traumatic left carotid cavernous fistula (CCF) with pseudoaneurysm of the left internal carotid artery. Brain magnetic resonance imaging (MRI) showed transiently restricted diffusion in the left centrum semiovale white matter and lower temporo-occipital area extending to the splenium of the corpus callosum, with high signal intensity on diffusion-weighted imaging. On the 35th day of admission, the patient had complete neurological recovery and a follow-up brain MRI revealed complete resolution of the lesions in the left centrum semiovale and splenium of the corpus callosum. These clinical and radiological features are highly suggestive of complete reversal of diffusion restriction after successful embolization of traumatic CCF.
MeSH Terms
Figure
-
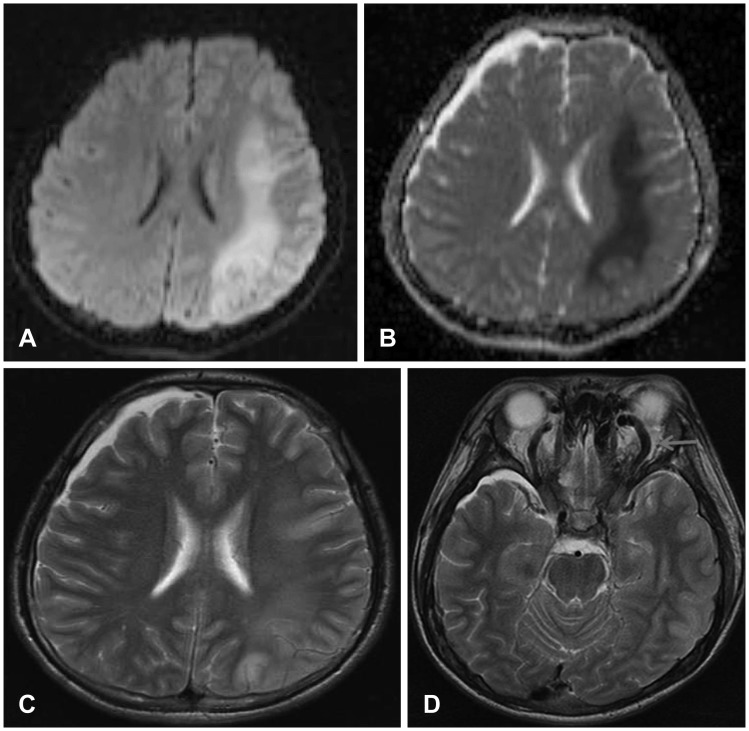
FIGURE 1 Diffusion weighted image (A) showing high signal intensity in the subcortical white matter of left centrum semiovale and lower temporo-occipital area. (B) Apparent diffusion coefficient map signal reduction is seen in the same region. (C) T2-weighted axial magnetic resonance imaging (MRI) demonstrating high signal intensity in the same region. (D) T2-weighted axial MRI demonstrating the dilated tortuous superior ophthalmic vein.
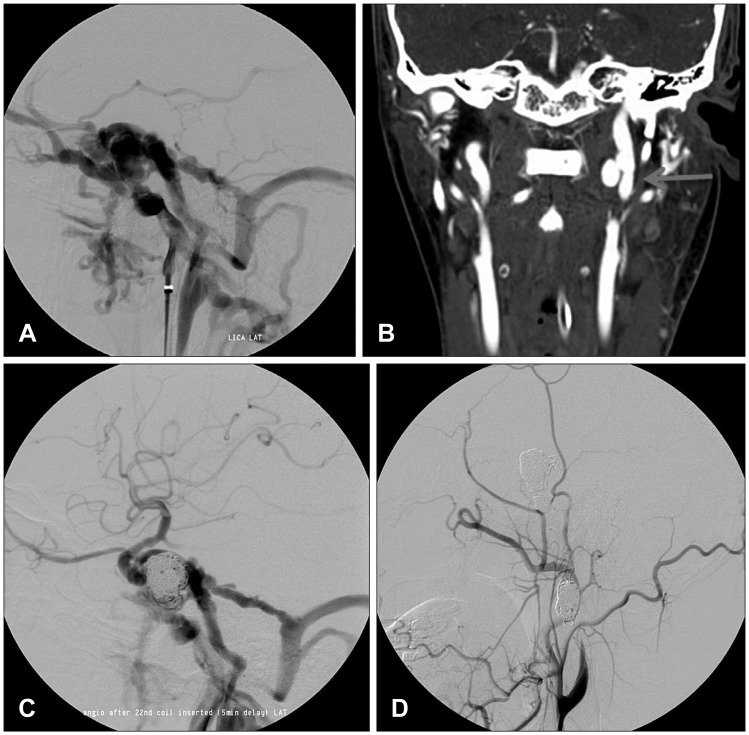
FIGURE 2 (A) Left internal carotid artery (ICA) angiogram showing a direct carotid cavernous fistula that drains into the superior ophthalmic vein, sphenoparietal sinus, and inferior petrosal sinus. (B) Intracranial computed tomography angiography demonstrating a large pseudoaneurysm arising from the left upper cervical ICA. (C) Postembolization angiography revealing a significant fistula flow into petrosal sinus. (D) Final angiography after second embolization showing complete occlusion of left ICA and a successful embolization of the pseudoaneurysm.
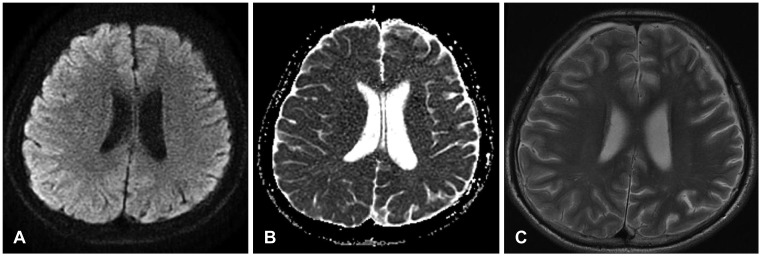
FIGURE 3 A 5-week follow-up (A) diffusion weighted image, (B) apparent diffusion coefficient map, and (C) T2-weighted image demonstrating complete reversal of diffusion restriction in the left centrum semiovale.
Reference
-
1. Al Brashdi YH, Albayram MS. Reversible restricted-diffusion lesion representing transient intramyelinic cytotoxic edema in a patient with traumatic brain injury. Neuroradiol J. 2015; 28:409–412. PMID: 26306930.
Article2. Aralasmak A, Karaali K, Cevikol C, Senol U, Sindel T, Toprak H, et al. Venous drainage patterns in carotid cavernous fistulas. ISRN Radiol. 2014; 2014:760267. PMID: 24967298.
Article3. Barut BO, Tascilar N, Aciman E, Acikgoz M, Ekem S. Carotid cavernous fistula with bilateral thalamic infarct. J Pak Med Assoc. 2012; 62:726–728. PMID: 23866525.4. Dabus G, Bernstein RA, Hurley MC, Shaibani A, Bendok BR, Russell EJ. Reversal of diffusion restriction after embolization of dural arteriovenous fistula: case report. Neurosurgery. 2010; 67:E1147–E1151. PMID: 20881533.
Article5. de Aguiar GB, Jory M, Silva JM, Conti ML, Veiga JC. Advances in the endovascular treatment of direct carotid-cavernous fistulas. Rev Assoc Med Bras (1992). 2016; 62:78–84. PMID: 27008498.6. Gist TL, Rangel-Castilla L, Krishna C, Roman GC, Cech DA, Diaz O. Endovascular management of six simultaneous intracranial dural arteriovenous fistulas in a single patient. J Neurointerv Surg. 2014; 6:e16. PMID: 23493339.
Article7. Ikeda G, Kato N, Watanabe D, Ogata A, Kasuya H, Yamazaki T, et al. A case of non-traumatic direct carotid-cavernous fistula presenting with cerebral infarction. No Shinkei Geka. 2012; 40:785–792. PMID: 22915700.8. Kaino K, Kumagai R, Furukawa S, Isono M, Muramatsu A, Fujii M, et al. Reversible splenial lesion syndrome with a hyperosmolar hyperglycemic state and neuroleptic malignant syndrome caused by olanzapine. J Diabetes Investig. 2017; 8:392–394.
Article9. Kim JG, Cho WS, Kang HS, Kim JE. Spontaneous carotid-cavernous fistula in the type IV ehlers-danlos syndrome. J Korean Neurosurg Soc. 2014; 55:92–95. PMID: 24653803.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Carotid-cavernous Fistula Bringing about Intracerebral Hemorrhage
- Bilateral Traumatic Carotid-Cavernous Fistula
- Regional Cerebral Blood Flow Changes in Traumatic Carotid Cavernous Fistula During Trapping Procedure: Case Study, Preliminary Report
- A Case of Spontaneous of Traumatic Carotid Cavernous Fistula After Carotid Angiography
- Direct Microsurgical Repair of Traumatic Carotid-Cavernous Fistula
