CT Findings of Immunoglobulin G4 Related Periaortitis and Periarterities: A Case Report
- Affiliations
-
- 1Department of Radiology, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Korea. haneul88@hanmail.net
- 2Department of Pathology, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Korea.
- 3Division of Cardiology, Department of Internal Medicine, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Korea.
- KMID: 2394048
- DOI: http://doi.org/10.3348/jksr.2017.77.5.333
Abstract
- Immunoglobulin G4 (IgG4)-related periaortitis and periarteritis are rare systemic inflammatory and fibrosclerosing diseases, usually involving the aorta and its main branches. We report a pathologically confirmed case of IgG4-related periaortitis involving the thoracoabdominal aorta, which can be confused with intramural hematoma or periaortic lymphoma.
MeSH Terms
Figure
-
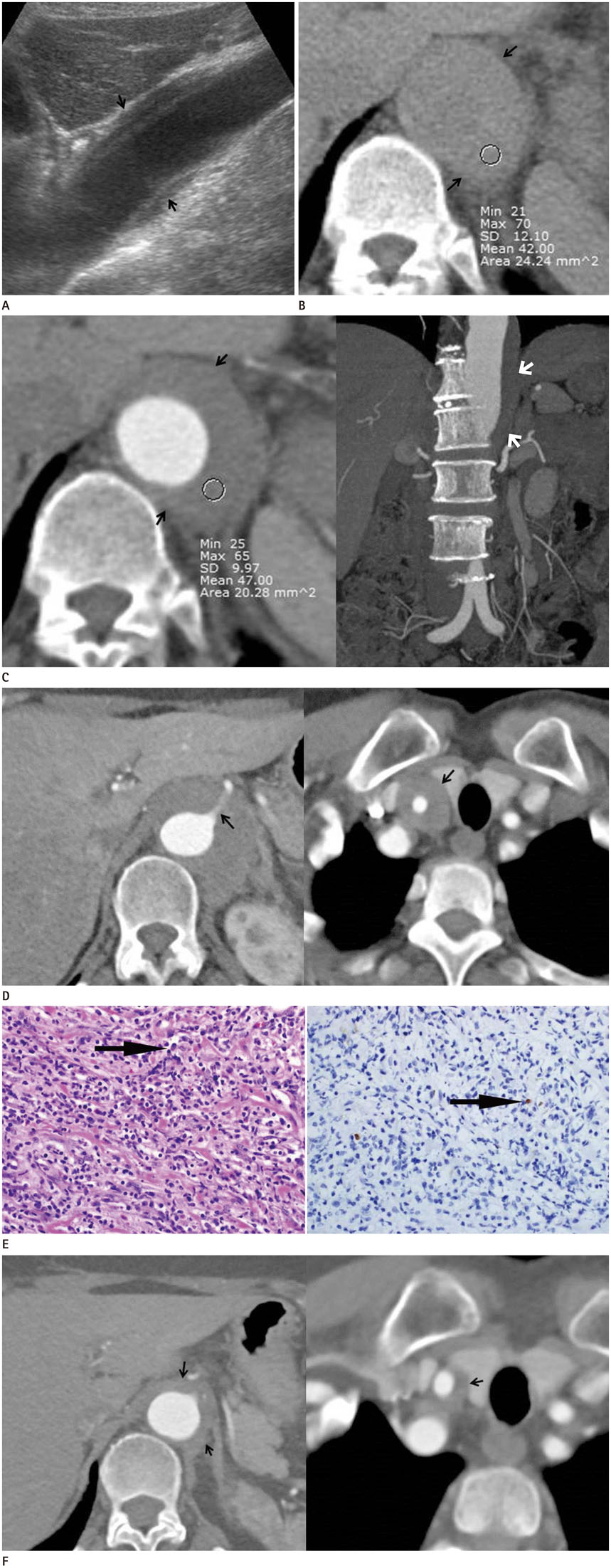
Fig. 1 A 63-year-old woman with IgG4-related periaortitis involving the thoracoabdominal aorta. A. Abdominal ultrasonography revealed localized eccentric hypoechoic aortic wall thickening (arrows, 11 mm in maximal thickness) at the upper abdominal aorta. The lesion seems to be a relatively preserved intima layer, and the thickening mainly occurs in the adventitia and only partly in the media layer of the aorta. B. On initial CTA, semi-circular eccentric, high-attenuated soft tissue lesion at the thoracoabdominal junction of the aorta (arrows) is seen on pre-enhanced axial image. The attenuation of the internal area is 42 HU. C. On initial post-enhanced axial and coronal CTA images, little homogenous enhancement (47 HU) with a smooth border at the same location (arrows), with thickening mainly in the adventitia and only partly in the media layer of the aorta is seen. The maximal wall thickness and longitudinal length of the lesion are about 11 and 105 mm, respectively. Notably, there is no distinct atherosclerotic change in the affected segment of the aorta, and no streaky infiltration around this lesion. CTA = computed tomography aortography, IgG4 = immunoglobulin G4, HU = Hounsfield unit, SD = standard deviation D. After two months, the aortic wall thickness at the thoracoabdominal junction area markedly increased from 11 to 18 mm. The proximal celiac artery enclosed within the lesion shows diffuse luminal narrowing (left arrow). Another prominent circumferential soft tissue lesion around the right proximal common carotid artery is noted (right arrow). E. Histologic specimens reveal diffuse lymphoplasmacytic cell infiltration and some eosinophils, suggesting chronic fibrosclerosing disorder (left arrow, hematoxylin and eosin stain, × 400). Immunochemical staining of IgG4 revealed elevated IgG4-positive plasma cells in the tissue, confirming IgG4-related periaortitis (right arrow, IgG4 immunohistochemical stain, × 400). IgG4 = immunoglobulin G4
Reference
-
1. Lipton S, Warren G, Pollock J, Schwab P. IgG4-related disease manifesting as pachymeningitis and aortitis. J Rheumatol. 2013; 40:1236–1238.2. Stone JH. L45. Aortitis, retroperitoneal fibrosis, and IgG4-related disease. Presse Med. 2013; 42(4 Pt 2):622–625.3. Mizushima I, Inoue D, Yamamoto M, Yamada K, Saeki T, Ubara Y, et al. Clinical course after corticosteroid therapy in IgG4-related aortitis/periaortitis and periarteritis: a retrospective multicenter study. Arthritis Res Ther. 2014; 16:R156.4. Babur Güler G, Cantürk E, Güler E, Oran G, Demir GG, Akçevin A, et al. IgG4-related aortitis mimicking intramural hematoma. Anatol J Cardiol. 2016; 16:728–729.5. Inoue D, Zen Y, Abo H, Gabata T, Demachi H, Yoshikawa J, et al. Immunoglobulin G4-related periaortitis and periarteritis: CT findings in 17 patients. Radiology. 2011; 261:625–633.6. Siddiquee Z, Smith RN, Stone JR. An elevated IgG4 response in chronic infectious aortitis is associated with aortic atherosclerosis. Mod Pathol. 2015; 28:1428–1434.7. Nishimura S, Amano M, Izumi C, Kuroda M, Yoshikawa Y, Takahashi Y, et al. Multiple coronary artery aneurysms and thoracic aortitis associated with IgG4-related disease. Intern Med. 2016; 55:1605–1609.8. Zambetti BR, Garrett E Jr. Plasmacytic aortitis with occlusion of the right coronary artery. Am J Case Rep. 2016; 17:549–552.9. Tran MN, Langguth D, Hart G, Heiner M, Rafter A, Fleming SJ, et al. IgG4-related systemic disease with coronary arteritis and aortitis, causing recurring critical coronary ischemia. Int J Cardiol. 2015; 201:33–34.10. Rousselin C, Pontana F, Puech P, Lambert M. [Differential diagnosis of aortitis]. Rev Med Interne. 2016; 37:256–263.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of IgG4-Related Disease with Pachymeningitis and Periaortitis
- Non-IgG4-Related Fibrosclerosing Periaortitis with Multisystemic Involvement
- Unusual Manifestation of Immunoglobulin G4-Related Disease Involving the Retroperitoneum: A Case Report
- A Rare Case of Granulomatosis with Polyangiitis-Related Periaortitis at the Ascending Aorta
- Immunoglobulin G4-Related Lung Disease Mimicking Lung Cancer: Two Case Reports
