Horizontal Stent Assisted Coiling of Wide Neck Basilar Tip Aneurysm: Comparison of Two Cases
- Affiliations
-
- 1Department of Neurosurgery, Cheongju St. Mary's Hospital, The Catholic University of Korea, Cheongju, Korea.
- 2Department of Neurosurgery, St. Vincent's Hospital, The Catholic University of Korea, Suwon, Korea. jaehoonsung@gmail.com
- KMID: 2393503
- DOI: http://doi.org/10.7461/jcen.2017.19.3.201
Abstract
- Currently, endovascular coiling is a popular treatment for basilar tip aneurysms, which usually involve a wide neck. Serious complications can occur when the posterior cerebral artery (PCA) originating from a wide neck is not properly preserved. Accordingly, various adjunctive procedures using stents or a balloon have been introduced. Herein we report two cases of basilar tip aneurysms in which retrograde horizontal (from one PCA to the other PCA) stent-assisted coiling was successful, and we provide a summary of the important technical points.
Keyword
MeSH Terms
Figure
-
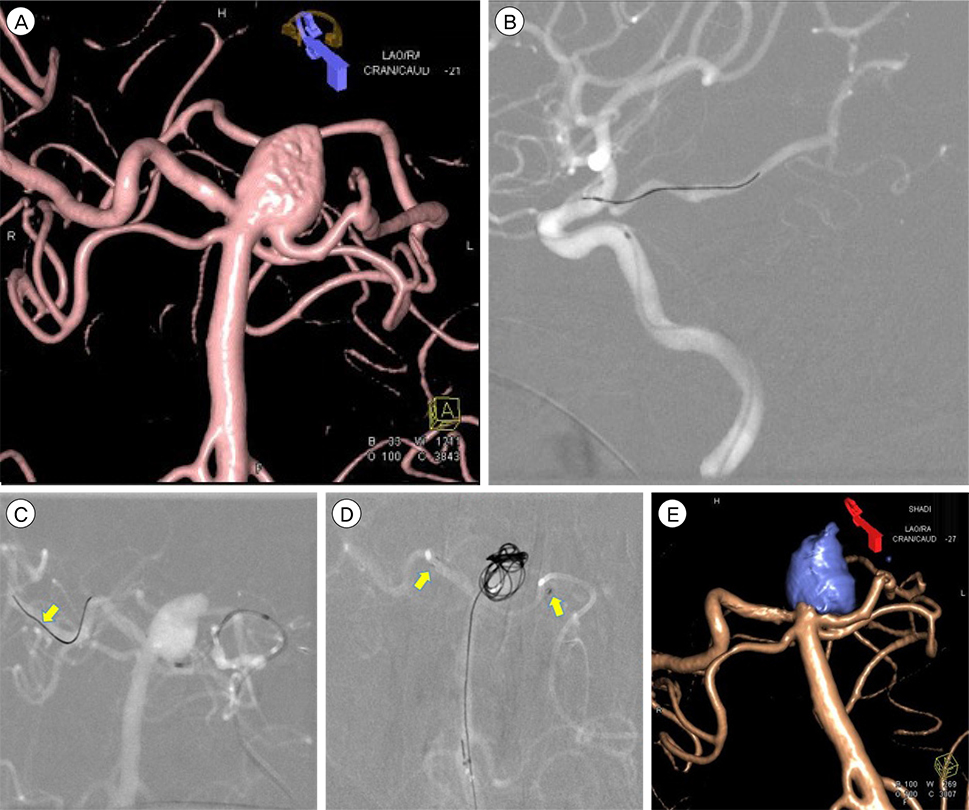
Fig. 1 Serial angiography images of Case 1. (A) The 3D angiography of case 1 shows saccular aneurysm at basilar tip. The height of aneurysm is about 9 mm. (B) The roadmap view of case 1 shows relatively straight course of left Pcom and PCA. The Pcom size is about 1.9 mm. Compared to case 2, the navigation of microwire (and subsequent) mirocatheter is relatively easy. (C) The roadmap view of case 1 shows one stage navigation of microwire to right distal PCA (arrow). The microcatheter is ready to cross the aneurysm neck. (D) The roadmap view of case 1 shows successful deployment of Enterprise stent (arrows) and subsequent coiling via double microcatheters from left vertebral artery. (E) The final 3D angiography of case 1 shows complete coil packing into aneurysm with excellent preservation of both PCAs. PCA = posterior cerebral artery.
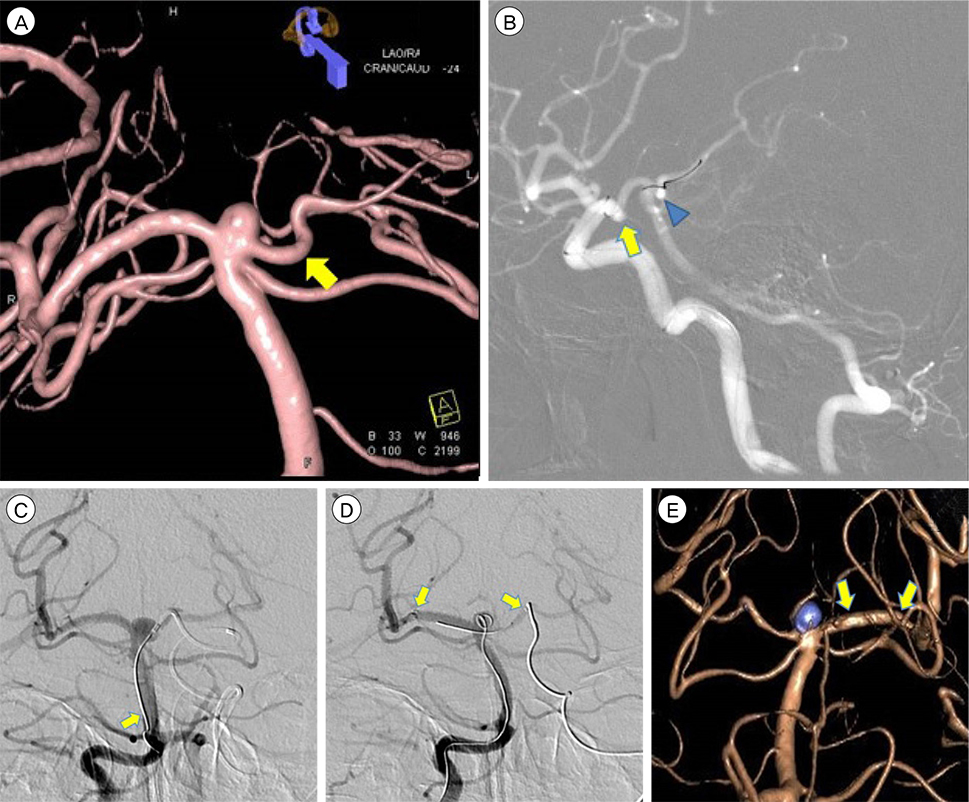
Fig. 2 Serial angiography images of Case 2. (A) The 3D angiography of case 2 shows small saccular aneurysm with at basilar tip. The height of aneurysm is about 2.8 mm. Compared to case 1, note the acute downward sagging course of left P1 segment (arrow), which make subsequent navigation difficult. (B) The roadmap view of case 2 shows V shaped kink of Pcom origin (arrow) and downward sagging of left P1 segment of PCA (triangle). They are big obstacle of navigation of mircowire and catheter. The Pcom size is over 2 mm. (C) The vertebral angiography of case 2 shows two stage navigation of microwire. The acute downward sagging of left P1 and short height of aneurysm make the microwire advance to proximal basilar artery firstly, rather than launch to right PCA directly (arrow). (D) The vertebral angiography of case 2 shows successful deployment of Enterprise stent (arrows) and partially deployed the 1st coil loop into aneurysm sac. After stent deployment, the downward sagging of left P1 is somewhat straightened. (E) The final 3D angiography of case 2 also shows complete packing. The inserted Enterprise stent makes the curved left PCA straight (arrows). PCA = posterior cerebral artery.
Cited by 1 articles
-
Endovascular Coiling for a Wide-neck Bifurcated Aneurysm with Anterograde Horizontal Stenting via Microcatheter Looping: A Technical Case Report
Hyun-Jae Jeon, Jong-Hwa Park, Jong-Young Lee, Hong-Jun Jeon, Seoung-Woo Park, Byung-Moon Cho
J Cerebrovasc Endovasc Neurosurg. 2018;20(3):181-186. doi: 10.7461/jcen.2018.20.3.181.
Reference
-
1. Akgul E, Aksungur E, Balli T, Onan B, Yilmaz DM, Bicakci S, et al. Y-stent-assisted coil embolization of wide-neck intracranial aneurysms. A single center experience. Interv Neuroradiol. 2011; 03. 17(1):36–48.2. Blackburn SL, Kadkhodayan Y, Shekhtman E, Derdeyn CP, Cross DT 3rd, Moran CJ. Treatment of basilar tip aneurysms with horizontal pca to pca stent-assisted coiling: Case series. J Neurointerv Surg. 2013; 05. 5(3):212–216.
Article3. Cross DT 3rd, Moran CJ, Derdeyn CP, Mazumdar A, Rivet D, Chicoine MM. Neuroform stent deployment for treatment of a basilar tip aneurysm via a posterior communicating artery route. AJNR Am J Neuroradiol. 2005; Nov-Dec. 26(10):2578–2581.4. Horowitz M, Levy E, Sauvageau E, Genevro J, Guterman LR, Hanel R, et al. Intra/extra-aneurysmal stent placement for management of complex and wide-necked-bifurcation aneurysms: Eight cases using the waffle cone technique. Neurosurgery. 2006; 04. 58:4 Suppl 2. ONS-258–ONS-262. discussion ONS-262.5. Liu W, Kung DK, Policeni B, Rossen JD, Jabbour PM, Hasan DM. Stent-assisted coil embolization of complex wide-necked bifurcation cerebral aneurysms using the “waffle cone” technique. A review of ten consecutive cases. Interv Neuroradiol. 2012; 03. 18(1):20–28.6. Moret J, Cognard C, Weill A, Castaings L, Rey A. The “remodelling technique” in the treatment of wide neck intracranial aneurysms. Angiographic results and clinical follow-up in 56 cases. Interv Neuroradiol. 1997; 03. 3(1):21–35.7. Xu X, Zheng Y, Wang D, Cui J, Shang X. Improved endovascular coiling of wide-neck intracranial aneurysms in elderly patients by double-microcatheter technique. Cell Biochem Biophys. 2015; 04. 71(3):1281–1286.8. Yashar P, Kan PT, Levy EI. Horizontal deployment of an intracranial stent via an antegrade approach for coil embolization of a basilar apex aneurysm: Technical note. J Neurointerv Surg. 2011; 12. 3(4):355–357.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Very Late Stent Thrombosis after Sole Stent-Assisted Coiling at the Paraclinoid Giant Aneurysm : Could Prophylactic Antiplatelet Therapy Be Ceased at the Only 1 Year after Procedure?
- Staged Y-shaped Stent Assisted Coil Embolization in a Wide-Neck Basilar Tip Aneurysm: Case Report
- Kissing Aneurysms at Fenestrated Proximal Basilar Artery: Double-barrel Stent-assisted Coiling Using Dual Closed-cell Stents
- Waffle-Cone Technique Using Solitaire AB Stent
- Y-Stenting Endovascular Treatment for Ruptured Intracranial Aneurysms : A Single-Institution Experience in Korea
