Rapid and Potent Antiarrhythmic Effect of Cardiac Resynchronization Therapy in a Patient with Advanced Dilated Cardiomyopathy and a Large Ventricular Arrhythmia Burden
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Dong-A University College of Medicine, Busan, Korea. thinkmed@dau.ac.kr
- KMID: 2392891
- DOI: http://doi.org/10.4070/kcj.2016.0361
Abstract
- We report a case demonstrating a rapid and potent antiarrhythmic effect of biventricular pacing. A 67-year-old male patient with dilated cardiomyopathy was admitted for heart failure. The initial surface electrocardiogram revealed a left bundle branch block with a QRS complex duration of 200 ms. Echocardiographic examination revealed a left ventricular ejection fraction of 16%, a left ventricular end-diastolic dimension of 91 mm, and marked interventricular dyssynchrony. Continuous rhythm monitoring revealed frequently-recurring non-sustained monomorphic ventricular tachycardia (VT). Polymorphic VT, which persisted for 27 seconds, occurred on the third day after admission, and the R on T phenomenon recurred every two to three days thereafter. Optimal medical therapy for four weeks failed to suppress the recurrence of ventricular arrhythmias or ameliorate heart failure. Cardiac resynchronization therapy was initiated for an anticipated antiarrhythmic effect of biventricular pacing. Three days after the initiation of biventricular pacing, the ventricular arrhythmias disappeared almost completely.
MeSH Terms
Figure
-
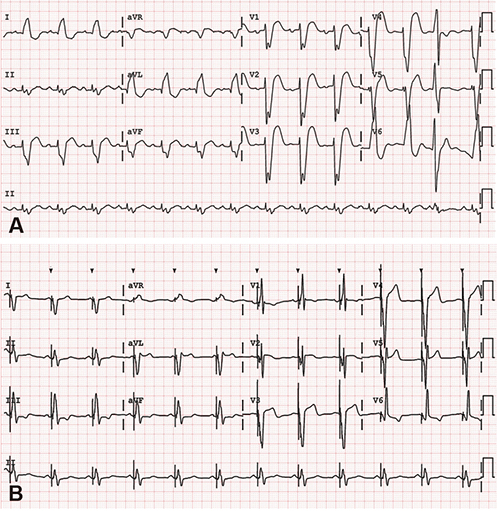
Fig. 1 Electrocardiographic findings before and after initiation of cardiac resynchronization therapy. (A) Initial electrocardiogram exhibits the sinus rhythm and notched broad QRS complexes with left bundle branch block configuration. The QRS complex duration was 200 ms, and the corrected QT interval calculated by Bazett's formula was 550 ms. (B) Follow-up electrocardiogram acquired during biventricular pacing exhibits shortening of the QRS complex duration from 200 to 160 ms and of the corrected QT interval from 550 to 500 ms. aVR: augmented voltage right arm, aVL: augmented voltage left arm, aVF: augmented voltage left foot.
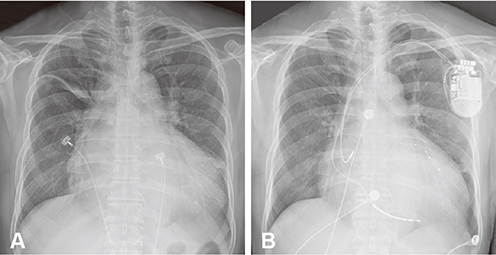
Fig. 2 Radiographic findings. (A) Initial chest X-ray displays cardiomegaly with a cardiac-thoracic ratio of 0.7 and minor fissural effusion. (B) Follow-up chest X-ray acquired 3 days after the initiation of cardiac resynchronization therapy displays a slight decrease in the cardiacthoracic ratio compared to the initial image.
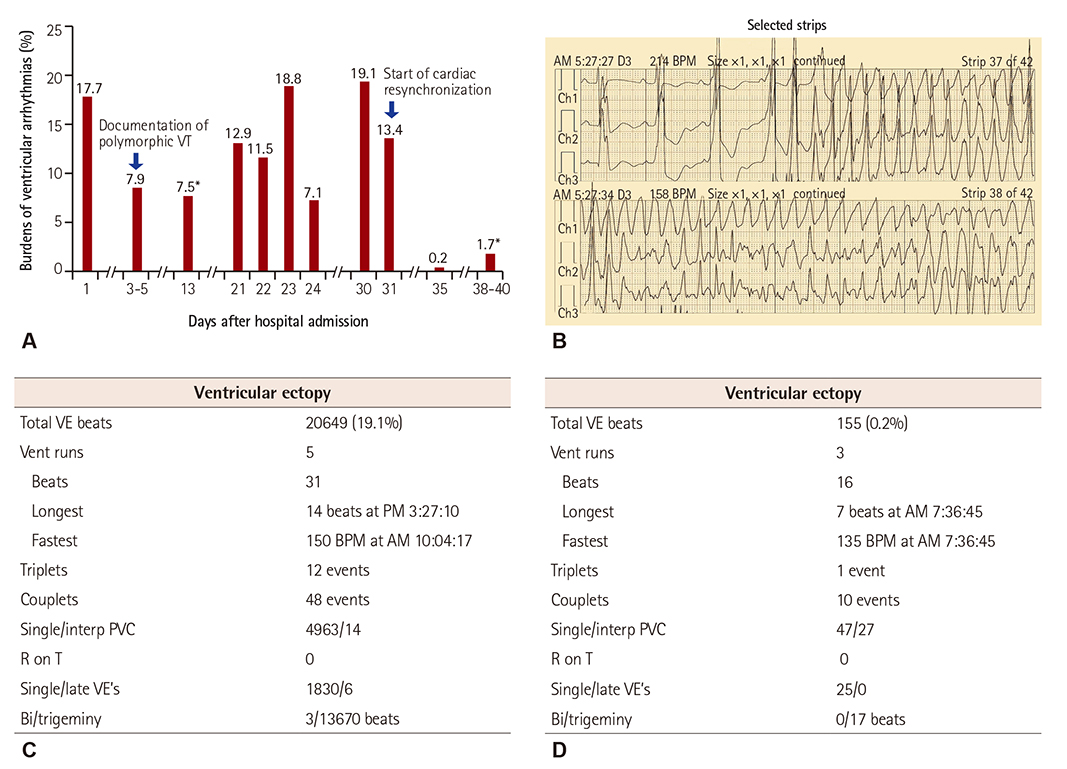
Fig. 3 Ventricular arrhythmia burden before and after initiation of cardiac resynchronization therapy. (A) The bar graph displays the daily or average (asterisk) burdens of ventricular arrhythmias, which were recorded by 24-hour or 72-hour ambulatory electrocardiographic monitoring according to the hospital admission days. (B) Data from 24-hour ambulatory electrocardiographic monitoring acquired 5 days after admission demonstrate the occurrence of polymorphic ventricular tachycardia, which persisted for 27 seconds and terminated spontaneously. (C) Analysis of the follow-up 24-hour ambulatory electrocardiographic monitoring data acquired one day before the initiation of cardiac resynchronization therapy displays a large burden of VPCs with multiple episodes of non-sustained monomorphic VT. Although optimal medical therapy was performed for over 4 weeks, the daily burden of ventricular arrhythmias was still 19% of the total daily beats. (D) Analysis of the follow-up 24-hour ambulatory electrocardiographic monitoring data acquired 3 days after the initiation of cardiac resynchronization therapy displays near complete disappearance of VPCs and VTs. The ventricular arrhythmia burden was reduced to 0.2% of the total daily beats. VT: ventricular tachycardia, VPC: ventricular premature complex, BPM: beat per minute, VE: ventricular ectopy, PVC: premature ventricular complex.
Reference
-
1. Meinertz T, Hofmann T, Kasper W, et al. Significance of ventricular arrhythmias in idiopathic dilated cardiomyopathy. Am J Cardiol. 1984; 53:902–907.2. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016; 18:891–975.3. Kies P, Bax JJ, Molhoek SG, et al. Effect of left ventricular remodeling after cardiac resynchronization therapy on frequency of ventricular arrhythmias. Am J Cardiol. 2004; 94:130–132.4. Di Biase L, Gasparini M, Lunati M, et al. Antiarrhythmic effect of reverse ventricular remodeling induced by cardiac resynchronization therapy: the InSync ICD (Implantable Cardioverter-Defibrillator) Italian Registry. J Am Coll Cardiol. 2008; 52:1442–1449.5. de Bakker JM, van Capelle FJ, Janse MJ, et al. Reentry as a cause of ventricular tachycardia in patients with chronic ischemic heart disease: electrophysiologic and anatomic correlation. Circulation. 1988; 77:589–606.6. Hamdan MH, Zagrodzky JD, Joglar JA, et al. Biventricular pacing decreases sympathetic activity compared with right ventricular pacing in patients with depressed ejection fraction. Circulation. 2000; 102:1027–1032.7. Kies P, Bax JJ, Molhoek SG, et al. Effect of cardiac resynchronization therapy on inducibility of ventricular tachyarrhythmias in cardiac arrest survivors with either ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol. 2005; 95:1111–1114.8. Ermis C, Seutter R, Zhu AX, et al. Impact of upgrade to cardiac resynchronization therapy on ventricular arrhythmia frequency in patients with implantable cardioverter-defibrillators. J Am Coll Cardiol. 2005; 46:2258–2263.9. Fish JM, Brugada J, Antzelevitch C. Potential proarrhythmic effects of biventricular pacing. J Am Coll Cardiol. 2005; 46:2340–2347.10. McSwain RL, Schwartz RA, DeLurgio DB, Mera FV, Langberg JJ, León AR. The impact of cardiac resynchronization therapy on ventricular tachycardia/fibrillation: an analysis from the combined Contak-CD and InSync-ICD studies. J Cardiovasc Electrophysiol. 2005; 16:1168–1171.11. Cha YM, Chareonthaitawee P, Dong YX, et al. Cardiac sympathetic reserve and response to cardiac resynchronization therapy. Circ Heart Fail. 2011; 4:339–344.12. Russo AM, Stainback RF, Bailey SR, et al. ACCF/HRS/AHA/ASE/HFSA/SCAI/SCCT/SCMR 2013 appropriate use criteria for implantable cardioverter-defibrillators and cardiac resynchronization therapy: a report of the American College of Cardiology Foundation appropriate use criteria task force, Heart Rhythm Society, American Heart Association, American Society of Echocardiography, Heart Failure Society of America, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance. Heart Rhythm. 2013; 10:e11–e58.13. Pinski SL, Fahy GJ. The proarrhythmic potential of implantable cardioverter-defibrillators. Circulation. 1995; 92:1651–1664.14. Runsio M, Kallner A, Kallner G, Rosenqvist M, Bergfeldt L. Myocardial injury after electrical therapy for cardiac arrhythmias assessed by troponin-T release. Am J Cardiol. 1997; 79:1241–1245.15. Goldenberg I, Moss AJ, Hall WJ, et al. Causes and consequences of heart failure after prophylactic implantation of a defibrillator in the multicenter automatic defibrillator implantation trial II. Circulation. 2006; 113:2810–2817.16. Poole JE, Johnson GW, Hellkamp AS, et al. Prognostic importance of defibrillator shocks in patients with heart failure. N Engl J Med. 2008; 359:1009–1017.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cardiac Resynchronization Therapy Defibrillator Treatment in a Child with Heart Failure and Ventricular Arrhythmia
- Recent Advancement in the Management of the Cardiac Arrhythmia
- A Case of Paroxymal Ventricular Tachycardia Improved due to Electrical Defibrillation was done Repeatedly in Patient with Ce rebral Infarction
- Reversal of Left Ventricular Function by PVC Ablation in Dilated Cardiomyopathy Patient
- Thoracoscopic Left Ventricular Lead Implantation in Cardiac Resynchronization Therapy
