Ann Rehabil Med.
2012 Oct;36(5):739-743.
Atypical Thoracic Solitary Plasmacytoma
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, College of Medicine, Kyung Hee University, Seoul 130-702, Korea. hdw1231@naver.com
- 2Department of Neurosurgery, College of Medicine, Kyung Hee University, Seoul 130-702, Korea.
- 3Department of Pathology, College of Medicine, Kyung Hee University, Seoul 130-702, Korea.
Abstract
- Plasmacytoma is a rare disease, which afflicts 2 to 3 people per every 100,000 of the general population. Solitary plasmacytoma accounts for 5% of the plasma cell neoplasm. Solitary plasmacytoma of the bone appears more vividly in the axial skeleton (25-60%), which has the red marrow and usually affects the thoracic vertebrae. We report a case of 54-year-old man who has a chest pain on the right side. After being treated for the muscle pain, his symptoms of pain were changed into weakness and allesthesia. We checked the MRI and found a mass lesion in the T5 vertebra, but there were no significant laboratory findings, in blood and urine samples. Finally, he got an operation due to the aggravation of the weakness. The result of biopsy indicated that it was a solitary plasmacytoma of the spine. After 5 months later, the weakness and allesthesia had disappeared.
MeSH Terms
Figure
-
Fig. 1 Anteroposterior (A) and lateral (B) x-rays in thoracic spine show non-specific findings.
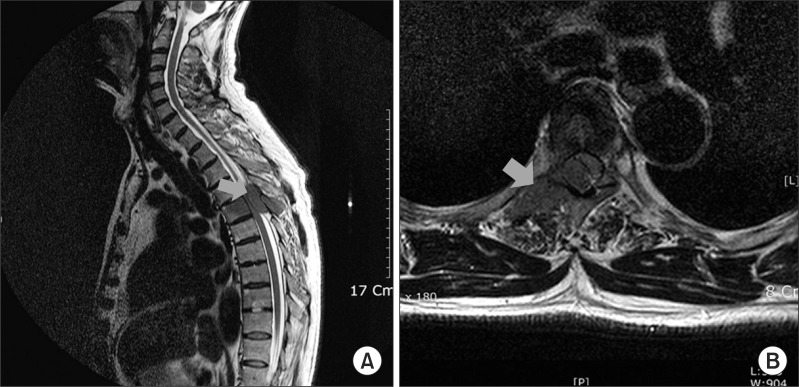
Fig. 2 T2 weighted MRIs show low signal changes like bone mass in sagittal view (A) and transverse view (B). These mass lesions show homogenous densities and slightly destructed cortex, red arrow: suspected mass lesions.
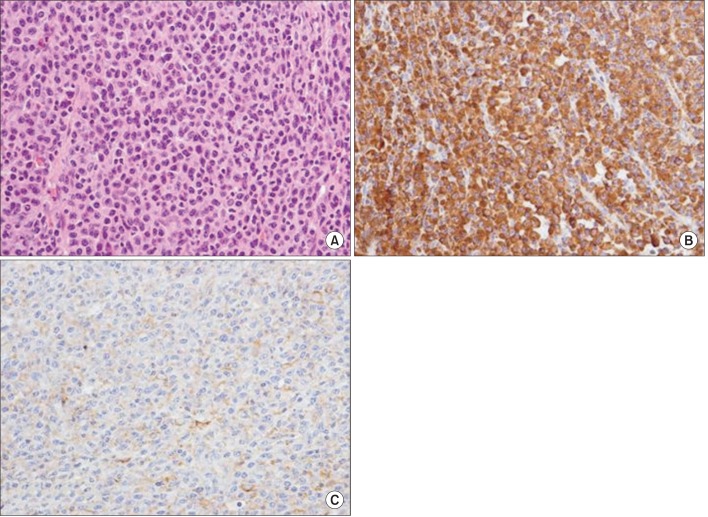
Fig. 3 It shows diffuse sheets of plasma cells (A). It shows diffuse cytoplasmic staining of kappa light chain (B) and negative reaction to lambda (C). These three histologic findings suggest plasmacytoma. (A) H&E (×400) (B, C) Immunohistochemistry stain (×400).
Reference
-
1. Schellinger KA, Propp JM, Villano JL, McCarthy BJ. Descriptive epidemiology of primary spinal cord tumors. J Neurooncol. 2008; 87:173–179. PMID: 18084720.
Article2. Taira H, Takasita M, Yoshida S, Tsumura H, Torisu T. Extraosseous calcified plasmacytoma causing thoracic myelopathy. Skeletal Radiol. 1999; 28:347–349. PMID: 10450883.
Article3. Takahashi T, Koshu K, Tominaga T, Takahashi A, Yoshimoto T. Solitary plasmacytoma in the thoracic spine. Two case reports. Neurosurg Rev. 1998; 21:121–125. PMID: 9795946.
Article4. Dimopoulos MA, Moulopoulos LA, Maniatis A, Alexanian R. Solitary plasmacytoma of bone and asymptomatic multiple myeloma. Blood. 2000; 96:2037–2044. PMID: 10979944.
Article5. Terada T. Solitary plasmacytoma of the thoracic vertebra presenting with sudden paraplegia and back pain: a pathologic case report. Pathol Oncol Res. 2011; 17:167–169. PMID: 20676811.6. Poor MM, Hitchon PW, Riggs CE Jr. Solitary spinal plasmacytomas: management and outcome. J Spinal Disord. 1988; 1:295–300. PMID: 2980978.7. Baba H, Maezawa Y, Furusawa N, Wada M, Kokubo Y, Imura S, Imamura Y, Yamada Y. Solitary plasmacytoma of the spine associated with neurological complications. Spinal Cord. 1998; 36:470–475. PMID: 9670382.
Article8. McLain RF, Weinstein JN. Solitary plasmacytoma of the spine: a review of 84 cases. J Spinal Disord. 1989; 2:69–74. PMID: 2520065.
