The Diagnosis of Metastatic Malignant Melanoma Incidentally Found during a National Health Screening Endoscopy: A Case Report
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea. endoksj@gmail.com
- KMID: 2391368
- DOI: http://doi.org/10.4166/kjg.2017.70.2.103
Abstract
- Malignant melanoma is one of the most common malignant diseases of the gastrointestinal tract. It has been reported that the malignant melanoma metastasizes not only to the small intestine due to the abundant blood supply, but also to the stomach, colon, and esophagus. Gastrointestinal metastasis is usually suspected depending on the clinical symptoms, as well as based on radiological or endoscopic findings. Imunohistochemical stains, such as Melan-A/Melanoma antigen recognized by T cell-1 or human melanoma black-45, are useful for confirming the diagnosis of malignant melanoma. A 44-year-old male received an operation due to a malignant melanoma at the left thumb two years ago. On the national health screening endoscopy, a submucosal tumor with hyperemic change on the top was found. The final diagnosis was a metastatic malignant melanoma in the stomach, pancreas, and pelvic bone. We recommend that endoscopists should consider the potential malignancy of subepithelial tumor with mucosa change, despite the tumor size being less than 1 cm.
Keyword
MeSH Terms
Figure
-
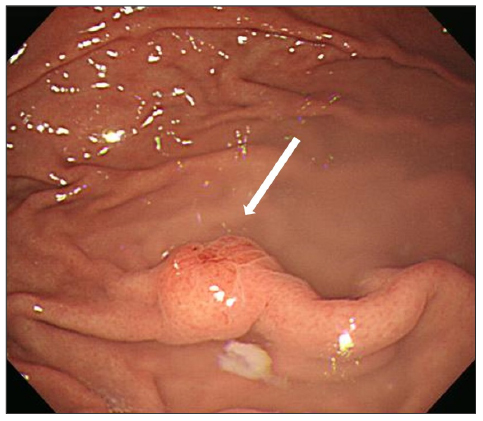
Fig. 1 Endoscopic finding. Subepithelial tumor-like lesion (8 mm) with hypervascular change on the fundus (arrow).
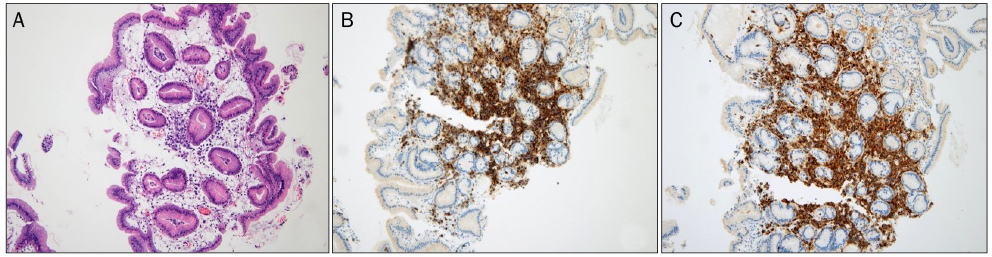
Fig. 2 Pathologic finding. (A) Abnormal cell proliferation is observed. The nuclei of the cells are larger than other inflammatory cells (H&E stain, ×100). (B) Strongly positive immunohistochemical stains for HMB-45 protein (HMB-45 stain, ×100). (C) Strongly positive immunohistochemical stains for Melan-A (Melan-A stain, ×100). HMB-45, human melanoma black-45.
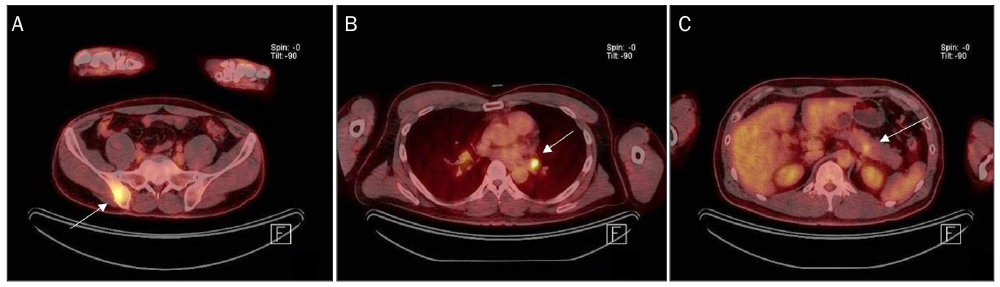
Fig. 3 PET-CT finding. (A) Increased FDG uptake at the right ilium (arrow). (B) Increased FDG uptake at the left hilar area in the mediastinum (arrow). (C) Focal increased FDG uptake at the pancreatic body (arrow). PET, photon emission tomography; CT, computed tomography; FDG, fluorodeoxyglucos.
Reference
-
1. Ryu JS, Oh HJ, Hu JW, et al. Two cases of endoscopically diagnosed gastric metastatic malignant melanoma of unknown origin. Korean J Gastrointest Endosc. 2004; 28:71–75.2. Ihde JK, Coit DG. Melanoma metastatic to stomach, small bowel, or colon. Am J Surg. 1991; 162:208–211.3. Caputy GG, Donohue JH, Goellner JR, Weaver AL. Metastatic melanoma of the gastrointestinal tract. Result of surgical management. Arch Surg. 1991; 126:1353–1358.4. Kadakia SC, Parker A, Canales L. Metastatic tumors to the upper gastrointestinal tract: endoscopic experience. Am J Gastroenterol. 1992; 87:1418–1423.5. Schuchter LM, Green R, Fraker D. Primary and metastatic diseases in malignant melanoma of the gastrointestinal tract. Curr Opin Oncol. 2000; 12:181–185.6. Horowitz M, Nobrega MM. Primary anal melanoma associated with melanosis of the upper gastrointestinal tract. Endoscopy. 1998; 30:662–665.7. McDermott VG, Low VH, Keogan MT, Lawrence JA, Paulson EK. Malignant melanoma metastatic to the gastrointestinal tract. AJR Am J Roentgenol. 1996; 166:809–813.8. Nelson RS, Lanza F. Malignant melanoma metastatic to the upper gastrointestinal tract: endoscopic and radiologic correlations, form and evolution of lesions, and value of directed biopsy in diagnosis. Gastrointest Endosc. 1978; 24:156–158.9. Markovic SN, Erickson LA, Rao RD, et al. Malignant melanoma in the 21st century, part 2: staging, prognosis, and treatment. Mayo Clin Proc. 2007; 82:490–513.10. Hodi FS, O'Day SJ, McDermott DF, et al. Improved survival with Ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010; 363:711–723.11. Robert C, Schachter J, Long GV, et al. Pembrolizumab versus Ipilimumab in advanced melanoma. N Engl J Med. 2015; 372:2521–2532.12. Cho JW. Korean ESD Study Group. Current guidelines in the management of upper gastrointestinal subepithelial tumors. Clin Endosc. 2016; 49:235–240.13. Lee NK, Kim S, Kim GH, et al. Hypervascular subepithelial gastrointestinal masses: CT-pathologic correlation. Radiographics. 2010; 30:1915–1934.
