An Electrode Configuration for Recording Muscle Motor Evoked Potentials in the Upper Extremities during Intraoperative Neurophysiological Monitoring
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. chungc@snu.ac.kr
- 2Neuroscience Research Institute, Seoul National University Medical Research Center, Seoul, Korea.
- 3Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea.
- 4Department of Brain and Cognitive Sciences, Seoul National University College of Natural Sciences, Seoul, Korea.
- KMID: 2387887
- DOI: http://doi.org/10.3340/jkns.2016.0506.006
Abstract
OBJECTIVE
The main aim of the present study is to examine the electrode configurations used to record the muscle motor evoked potential (mMEP) in the upper extremities during surgery with the goal of producing a high and stable mMEP signal, in particular among the abductor pollicis brevis (APB), abductor digiti minimi (ADM), and across the APB-ADM muscles, which have been widely used for the mMEP in the upper extremities.
METHODS
Thirty right-handed patients were recruited in this prospective study. No patients showed any adverse events in their mMEP signals of the upper extremities during surgery. The mMEPs were recorded independently from the signals for the APB and ADM and for those across the APB-ADM.
RESULTS
The mMEP amplitude from across the APB-ADM was statistically higher than those recorded from the APB and ADM muscles. Moreover, the coefficient of variation of the mMEP amplitude from across the APB-ADM was smaller than those of mMEP amplitude recorded from the APB and ADM muscles.
CONCLUSION
The mMEP from across the APB-ADM muscles showed a high yield with high stability compared to those in each case from the APB and ADM muscles. The configuration across the APB-ADM muscles would be best for mMEP recordings from the upper extremities for intraoperative neurophysiological monitoring purposes.
Keyword
MeSH Terms
Figure
-

Fig. 1 Example of mMEP recorded from APB, ADM and across the APB-ADM muscles. The columns from left to right show mMEPs as recorded from the across-APB-ADM, APB and ADM locations, respectively. The mMEPs at 12:29:11 correspond to the mMEPs under a muscle relaxant. The mMEPs at 13:50:19 correspond to the baseline mMEPs, with the following mMEPs measured during surgery. The mMEP amplitudes recorded across APB-ADM muscles were the largest compared to the remaining recording sites, and the morphology appeared to be relatively consistent over time. mMEP: motor evoked potential, APB: abductor pollicis brevis, ADM: abductor digiti minimi.

Fig. 2 Boxplot of the mMEP amplitude recorded from the APB, ADM and across the APB-ADM muscles. The y-axis indicates the mMEP amplitude (unit: μV). Median mMEP amplitude values recorded from the APB, ADM and across the APB-ADM were 1853.9 μV, 893.0 μV, 2238.0 μV, respectively. Wilcoxon signed-rank tests with Bonferroni correction showed significant differences between APB and ADM (*p<0.01, r=0.74) and between the ADM and across-APB-ADM values (†p<0.01, r=0.83). But between the APB and across-APB-ADM values, there were not showed significant differences (‡p<0.05, r=0.49). mMEP: motor evoked potential, APB: abductor pollicis brevis, ADM: abductor digiti minimi.
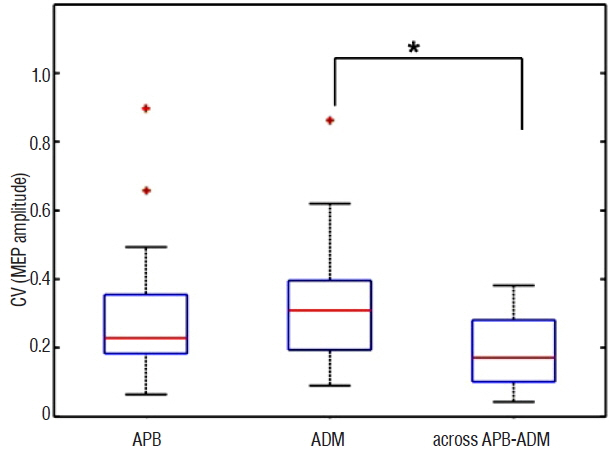
Fig. 3 Boxplot of the coefficient of variation (CV) of the mMEP amplitudes recorded from the APB and ADM and from across the APB-ADM muscles. The median CV of recorded from the APB, ADM and across-APB-ADM locations were 0.23, 0.31, and 0.17, respectively. Wilcoxon signed-rank tests with Bonferroni correction showed a larger amplitude recorded from across the APB-ADM muscles compared to that recorded from ADM (*p<0.01, r=0.65). No significant differences were detected between APB and ADM and between APB and across the APB-ADM. mMEP: motor evoked potential, APB: abductor pollicis brevis, ADM: abductor digiti minimi.
Reference
-
References
1. Mendiratta Anil, Emerson RG. Transcranial electrical mMEP with muscle recording. Nuwer MR, editor. Intraoperative Monitoring of Neural Function. Amsterdam: ELSEVIER;2008. p. 260–272.2. Deletis V, Sala F. Corticospinal tract monitoring with D- and I-waves from the spinal cord and muscle MEPs from limb muscles. Nuwer MR, editor. Intraoperative Monitoring of Neural Function. Amsterdam: ELSEVIER;2008. p. 235–251.
Article3. Jankowska E, Padel Y, Tanaka R. Projections of pyramidal tract cells to alpha-motoneurones innervating hind-limb muscles in the monkey. J Physiol. 249:637–667. 1975.
Article4. Kim SM, Yang H, Park SB, Han SG, Park KW, Yoon SH, et al. Pattern-specific changes and discordant prognostic values of individual leg-muscle motor evoked potentials during spinal surgery. Clin Neurophysiol. 123:1465–1470. 2012.
Article5. Macdonald DB, Stigsby B, Al Homoud I, Abalkhail T, Mokeem A. Utility of motor evoked potentials for intraoperative nerve root monitoring. J Clin Neurophysiol. 29:118–125. 2012.
Article6. Nuwer MR. Overview and history. Nuwer MR, editor. Intraoperative Monitoring of Neural Function. Amsterdam: ELSEVIER;2008. p. 2–6.
Article7. Thickbroom GW, Byrnes ML, Archer SA, Mastaglia FL. Motor outcome after subcortical stroke: MEPs correlate with hand strength but not dexterity. Clin Neurophysiol. 113:2025–2029. 2002.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative Neurophysiologic Monitoring: Basic Principles and Recent Update
- Monitoring of Motor and Somatosensory Evoked Potentials During Spine Surgery: Intraoperative Changes and Postoperative Outcomes
- Intraoperative Neurophysiological Monitoring for Spinal Cord Tumor Surgery: Comparison of Motor and Somatosensory Evoked Potentials According to Tumor Types
- Early Detection of the Internal Capsule Infarction by Intraoperative Neuromonitoring in Mesial Temporal Epilepsy Surgery
- Intraoperative Monitoring for Tethered Cord Syndrome Using Somatosensory Evoked Potential and Motor Evoked Potential: Report of three cases
