Correlation between MRI Grading System and Surgical Findings for Lumbar Foraminal Stenosis
- Affiliations
-
- 1Department of Neurosurgery, Gachon University Gil Medical Center, Incheon, Korea. ns-ay@hanmail.net
- 2Department of Radiology, Nanoori Hospital, Seoul, Korea.
- KMID: 2387885
- DOI: http://doi.org/10.3340/jkns.2016.1010.004
Abstract
OBJECTIVE
Magnetic resonance imaging (MRI) grading systems using sagittal images are useful for evaluation of lumbar foraminal stenosis. We evaluated whether such a grading system is useful as a diagnostic tool for surgery.
METHODS
Between July 2014 and June 2015, 99 consecutive patients underwent unilateral lumbar foraminotomy for lumbar foraminal stenosis. Surgically confirmed foraminal stenosis and the contralateral, asymptomatic neuroforamen were assessed based on a 4-point MRI grading system. Two experienced researchers independently evaluated the MR sagittal images. Interobserver agreement and intraobserver agreement were analyzed using κ statistics.
RESULTS
The mean age of patients (54 women, 45 men) was 62.5 years. A total of 101 levels (202 neuroforamens) were evaluated. MRI grades for operated neuroforamens were as follows: Grade 0 in 0.99%, Grade 1 in 5.28%, Grade 2 in 14.85%, and Grade 3 in 78.88%. Interobserver agreement was moderate for operated neuroforamens (κ=0.511) and good for asymptomatic neuroforamens (κ=0.696). Intraobserver agreement by reader 1 for operated neuroforamens was good (κ=0.776) and that for asymptomatic neuroforamens was very good (κ=0.831). In terms of lumbar level, interobserver agreement for L5-S1 (κ=0.313, fair) was relatively lower than the other level (κ=0.804, very good).
CONCLUSION
MRI grading system for lumbar foraminal stenosis is thought to be useful as a diagnostic tool for surgery in the lumbar spine; however, it is less reliable for symptomatic L5-S1 foraminal stenosis than for other levels. Thus, various clinical factors as well as the MRI grading system are required for surgical decision-making.
MeSH Terms
Figure
-
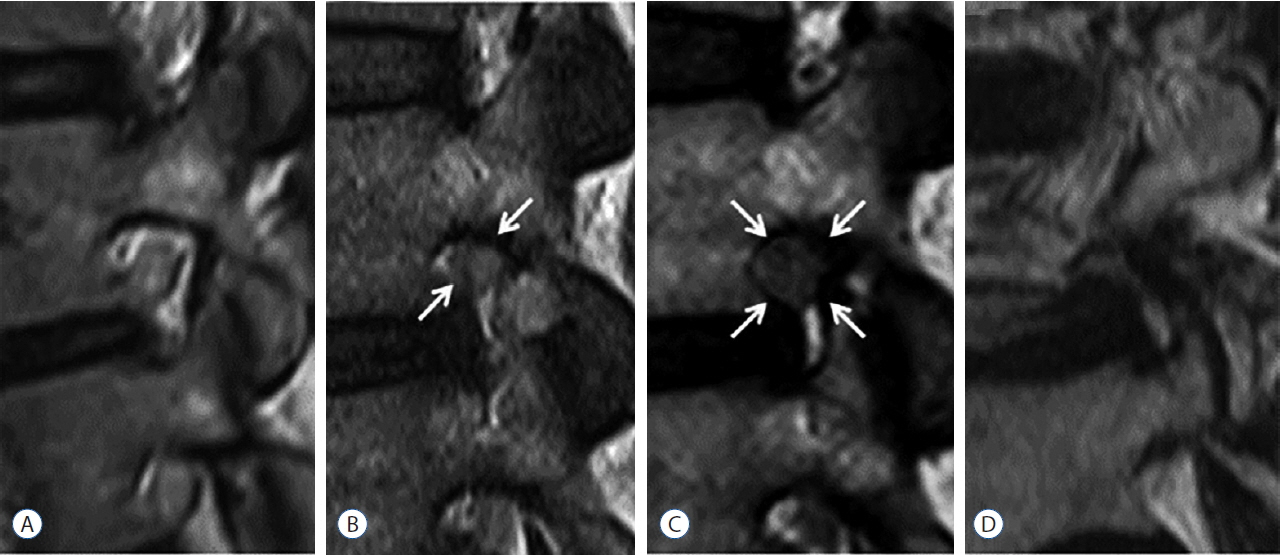
Fig. 1 Four-point-scale for grading of lumbar foraminal stenosis in sagittal MRI suggested by Lee et al.9). A: Grade 0 (normal). Sagittal cross section through foramen shows normal neuroforamen. B: Grade 1 (mild foraminal stenosis). Sagittal cross section through foramen shows perineural fat obliteration in two opposing directions (vertical or transverse, arrows). C: Grade 2 (moderate foraminal stenosis). Sagittal cross section through foramen shows perineural fat obliteration in four directions (arrows). D: Grade 3 (severe foraminal stenosis). Sagittal cross section through foramen shows morphologic changes in the nerve root. MRI: magnetic resonance imaging.

Fig. 2 T1-weighted sagittal image of a 44-year-old man with left lower extremity pain. A: Sagittal MR image shows Grade 3 foraminal stenosis at left foramen of the L3–L4 level. B: Sagittal MR image shows Grade 0 of normal neuroforamen at right foramen of the L3–L4 level. MR: magnetic resonance.
Reference
-
References
1. Attias N, Hayman A, Hipp JA, Noble P, Esses SI. Assessment of magnetic resonance imaging in the diagnosis of lumbar spine foraminal stenosis--a surgeon’s perspective. J Spinal Disord Tech. 19:249–256. 2006.
Article2. Chang SB, Lee SH, Ahn Y, Kim JM. Risk factor for unsatisfactory outcome after lumbar foraminal and far lateral microdecompression. Spine (Phila Pa 1976). 31:1163–1167. 2006.
Article3. Fujiwara A, An HS, Lim TH, Haughton VM. Morphologic changes in the lumbar intervertebral foramen due to flexion-extension, lateral bending, and axial rotation: an in vitro anatomic and biomechanical study. Spine (Phila Pa 1976). 26:876–882. 2001.
Article4. Grenier N, Kressel HY, Schiebler ML, Grossman RI, Dalinka MK. Normal and degenerative posterior spinal structures: MR imaging. Radiology. 165:517–525. 1987.
Article5. Hasegawa T, An HS, Haughton VM, Nowicki BH. Lumbar foraminal stenosis: critical heights of the intervertebral discs and foramina. A cryo-microtome study in cadavera. J Bone Joint Surg Am. 77:32–38. 1995.6. Jenis LG, An HS. Spine update. Lumbar foraminal stenosis. Spine (Phila Pa 1976). 25:389–394. 2000.7. Kunogi J, Hasue M. Diagnosis and operative treatment of intraforaminal and extraforaminal nerve root compression. Spine (Phila Pa 1976). 16:1312–1320. 1991.
Article8. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 33:159–174. 1977.
Article9. Lee S, Lee JW, Yeom JS, Kim KJ, Kim HJ, Chung SK, et al. A practical MRI grading system for lumbar foraminal stenosis. AJR Am J Roentgenol. 194:1095–1098. 2010.
Article10. Porter R, Hibbert C, Evans C. The natural history of root entrapment syndrome. Spine (Phila Pa 1976). 9:418–421. 1984.
Article11. Shim YJ, Ha HG, Lee JS, Kim YS, Park MS, Kim JS. Microsurgical decompression for lumbar stenosis via unilateral laminotomy. J Korean Neurosurg Soc. 29:1505–1513. 2000.12. Wildermuth S, Zanetti M, Duewell S, Schmid MR, Romanowski B, Benini A, et al. Lumbar spine: quantitative and qualitative assessment of positional (upright flexion and extension) MR imaging and myelography. Radiology. 207:391–398. 1998.
Article13. Zindrick MR, Wiltse LL, Doornik A, Widell EH, Knight GW, Patwardhan AG, et al. Analysis of the morphometric characteristics of the thoracic and lumbar pedicles. Spine (Phila Pa 1976). 12:160–166. 1987.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Magnetic Resonance Imaging Grading Systems for Central Canal and Neural Foraminal Stenoses of the Lumbar and Cervical Spines With a Focus on the Lee Grading System
- Can Conventional Magnetic Resonance Imaging Substitute Three-Dimensional Magnetic Resonance Imaging in the Diagnosis of Lumbar Foraminal Stenosis?
- Minimally Invasive Combined Interlaminar and Paraisthmic Approach for Symptomatic Lumbar Foraminal Stenosis : Surgical Technique and Preliminary Results
- To Assess Whether Lee’s Grading System for Central Lumbar Spinal Stenosis Can Be Used as a Decision-Making Tool for Surgical Treatment
- Percutaneous Stenoscopic Lumbar Decompression with Paramedian Approach for Foraminal/Extraforaminal Lesions
