Changes in Coronary Perfusion after Occlusion of Coronary Arteries in Kawasaki Disease
- Affiliations
-
- 1Department of Pediatrics, Myongji Hospital, Goyang, Korea.
- 2Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. amyjys@naver.com
Abstract
- PURPOSE
Myocardial infarction in children with total occlusion of a coronary artery after Kawasaki disease is rare due to multiple collateral vessels. We aimed to investigate the changes in coronary perfusion associated with coronary artery occlusion after Kawasaki disease.
MATERIALS AND METHODS
Eleven patients with coronary artery occlusion after Kawasaki disease were investigated. Serial coronary angiographies after total occlusion of a coronary artery were reviewed and the changes were described in all patients with additive information collected.
RESULTS
The median age at the occlusion was 5.9 years old. The interval to occlusion was 6.2+/-6.9 years. Four left anterior descending coronary artery total occlusions and 10 right coronary artery total occlusions were detected. Immediate coronary artery bypass graft for left anterior descending coronary artery total occlusion made right coronary total occlusion occurred in all except one patient and the intervals thereof were 1 year, 1.8 years, and 4 years. Collaterals to the left coronary artery regressed after recanalization, while new collaterals to the right coronary artery developed. In three, collaterals to the right coronary artery decreased without recanalization without clinical signs.
CONCLUSION
The right coronary artery should be followed up carefully because of possible occlusion of new onset or changes in collaterals.
MeSH Terms
Figure
-
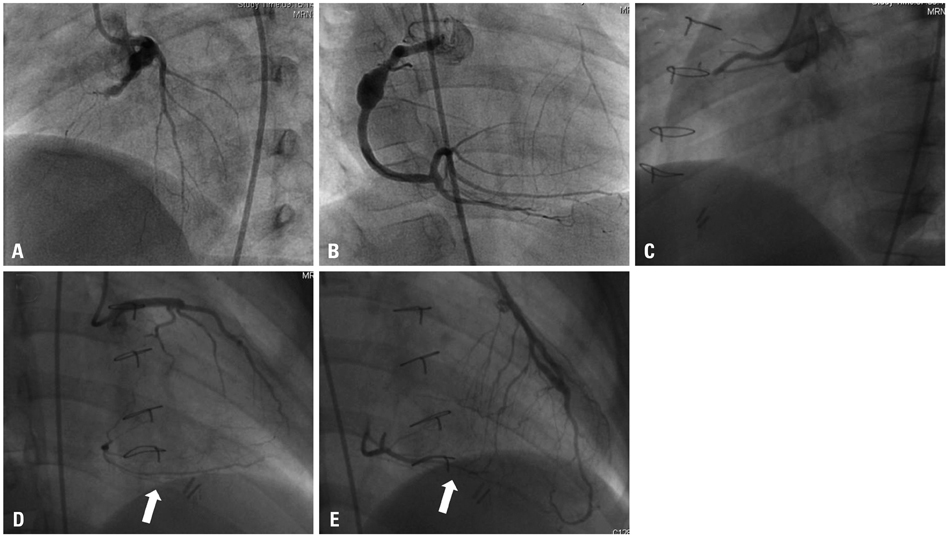
Fig. 1 (Patient 4) Kawasaki disease was diagnosed at the age of 5 years and his first coronary angiography at the age of 5.9 years showed total occlusion of the LAD (A). RCA angiogram showed aneurysm and collaterals to the LAD (B). The next coronary angiography was performed 6 months after coronary artery bypass graft to the LAD and showed RCA total occlusion (C), collaterals from left circumflex coronary artery (arrow) (D), and CABG flow to left anterior descending coronary artery (arrow) (E). LAD, left anterior descending coronary artery; RCA, right coronary artery; CABG, coronary artery bypass graft.
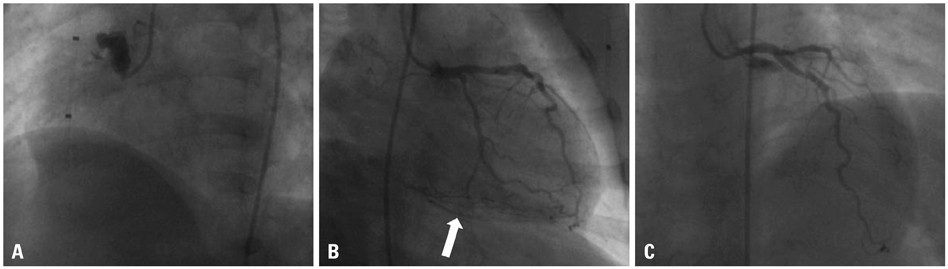
Fig. 2 (Patient 10) Kawasaki disease was diagnosed at the age of 3 months. His first coronary angiography was performed at the age of 1.5 years and showed right coronary artery total occlusion (A) with collaterals from left coronary artery (arrow) (B). Coronary angiography performed 1 year later demonstrated decrease in collaterals to the right coronary artery from the left coronary artery (C).
Reference
-
1. Ortiz-Pérez JT, Rodríguez J, Meyers SN, Lee DC, Davidson C, Wu E. Correspondence between the 17-segment model and coronary arterial anatomy using contrast-enhanced cardiac magnetic resonance imaging. JACC Cardiovasc Imaging. 2008; 1:282–293.
Article2. Kato H, Sugimura T, Akagi T, Sato N, Hashino K, Maeno Y, et al. Long-term consequences of Kawasaki disease. A 10- to 21-year follow-up study of 594 patients. Circulation. 1996; 94:1379–1385.3. Suzuki A, Kamiya T, Ono Y, Kinoshita Y, Kawamura S, Kimura K. Clinical significance of morphologic classification of coronary arterial segmental stenosis due to Kawasaki disease. Am J Cardiol. 1993; 71:1169–1173.
Article4. Shiraishi I, Onouchi Z, Hayano T, Hamaoka K, Kiyosawa N. Asymptomatic myocardial infarction in Kawasaki disease: long-term prognosis. Pediatr Cardiol. 1991; 12:78–82.
Article5. Tsuda E, Kitamura S. National survey of coronary artery bypass grafting for coronary stenosis caused by Kawasaki disease in Japan. Circulation. 2004; 110:11 Suppl 1. II61–II66.
Article6. Kitamura S, Tsuda E, Kobayashi J, Nakajima H, Yoshikawa Y, Yagihara T, et al. Twenty-five-year outcome of pediatric coronary artery bypass surgery for Kawasaki disease. Circulation. 2009; 120:60–68.
Article7. Onouchi Z, Hamaoka K, Kamiya Y, Hayashi S, Ohmochi Y, Sakata K, et al. Transformation of coronary artery aneurysm to obstructive lesion and the role of collateral vessels in myocardial perfusion in patients with Kawasaki disease. J Am Coll Cardiol. 1993; 21:158–162.
Article8. Kinoshita Y, Suzuki A, Nakajima T, Ono Y, Arakaki Y, Kamiya T. Collateral vessels assessed by myocardial contrast echocardiography in patients with coronary artery lesions after Kawasaki disease. Heart Vessels. 1996; 11:203–210.
Article9. TIMI Study Group. The Thrombolysis in Myocardial Infarction (TIMI) trial. Phase I findings. N Engl J Med. 1985; 312:932–936.10. Gibson CM, Cannon CP, Daley WL, Dodge JT Jr, Alexander B Jr, Marble SJ, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation. 1996; 93:879–888.11. Cohen M, Rentrop KP. Limitation of myocardial ischemia by collateral circulation during sudden controlled coronary artery occlusion in human subjects: a prospective study. Circulation. 1986; 74:469–476.
Article12. Fukuda T, Ishibashi M, Shinohara T, Miyake T, Kudoh T, Saga T. Follow-up assessment of the collateral circulation in patients with Kawasaki disease who underwent dipyridamole stress technetium-99m tetrofosmin scintigraphy. Pediatr Cardiol. 2005; 26:558–564.
Article13. Tatara K, Murata M, Itoh K, Kazuma N, Kondo C. Management of severe coronary sequelae of Kawasaki disease. Am Heart J. 1996; 131:576–581.
Article14. Kashyap R, Mittal BR, Bhattacharya A, Manojkumar R, Singh S. Exercise myocardial perfusion imaging to evaluate inducible ischaemia in children with Kawasaki disease. Nucl Med Commun. 2011; 32:137–141.
Article15. Kato H, Ichinose E, Kawasaki T. Myocardial infarction in Kawasaki disease: clinical analyses in 195 cases. J Pediatr. 1986; 108:923–927.
Article16. Suzuki A, Miyagawa-Tomita S, Nakazawa M, Yutani C. Remodeling of coronary artery lesions due to Kawasaki disease: comparison of arteriographic and immunohistochemical findings. Jpn Heart J. 2000; 41:245–256.17. Sabia PJ, Powers ER, Ragosta M, Sarembock IJ, Burwell LR, Kaul S. An association between collateral blood flow and myocardial viability in patients with recent myocardial infarction. N Engl J Med. 1992; 327:1825–1831.
Article18. Ishii M, Ueno T, Ikeda H, Iemura M, Sugimura T, Furui J, et al. Sequential follow-up results of catheter intervention for coronary artery lesions after Kawasaki disease: quantitative coronary artery angiography and intravascular ultrasound imaging study. Circulation. 2002; 105:3004–3010.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Right Coronary Arterial Occlusion with Normal Electrocardiogram in Atypical Kawasaki Diseases
- Kawasaki Disease
- Thrombolytic Therapy and Long Term Follow-up Study in a Child with Kawasaki Disease Complicated by Giant Coronary Aneurysm with Thrombosis
- Percutaneous Transluminal Coronary Angioplasty for Coronary Artery Stenosis in an Adult Kawasaki Disease with Coronary Aneurysm : A Case Report and Review
- A Clinical Observation of Kawasaki Disease at High Risk of Coronary Artery Aneurysm
