J Rheum Dis.
2017 Jun;24(3):157-160. 10.4078/jrd.2017.24.3.157.
A Case of Refractory Oral Aphthous Ulcer Successfully Treated with Adalimumab
- Affiliations
-
- 1Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea. sungyk@hanyang.ac.kr
- 2Department of Rheumatology, Keimyung University Dongsan Medical Center, Daegu, Korea.
- 3Department of Rheumatology, Hanyang University Hospital for Rheumatic Diseases, Seoul, Korea.
- KMID: 2385343
- DOI: http://doi.org/10.4078/jrd.2017.24.3.157
Abstract
- Oral aphthous ulcer is a common lesion characterized by loss of dermal tissue of various shapes in many diseases. It is not serious, but may affect quality of life through pain and discomfort. In many cases, it heals spontaneously without treatment or with topical agents such as antiseptics, analgesics and corticosteroid in a few days. However, rarely, there are a few cases of aphthous ulcer that remain refractory despite appropriate treatment. Tumor necrosis factor-α inhibitors have recently been used in treatment of severe mucosal ulcer in Behçet's disease. Herein, we report a patient suffering from refractory oral aphthous ulcers that were resistant to topical and systemic agents, but were successfully treated with adalimumab.
MeSH Terms
Figure
-
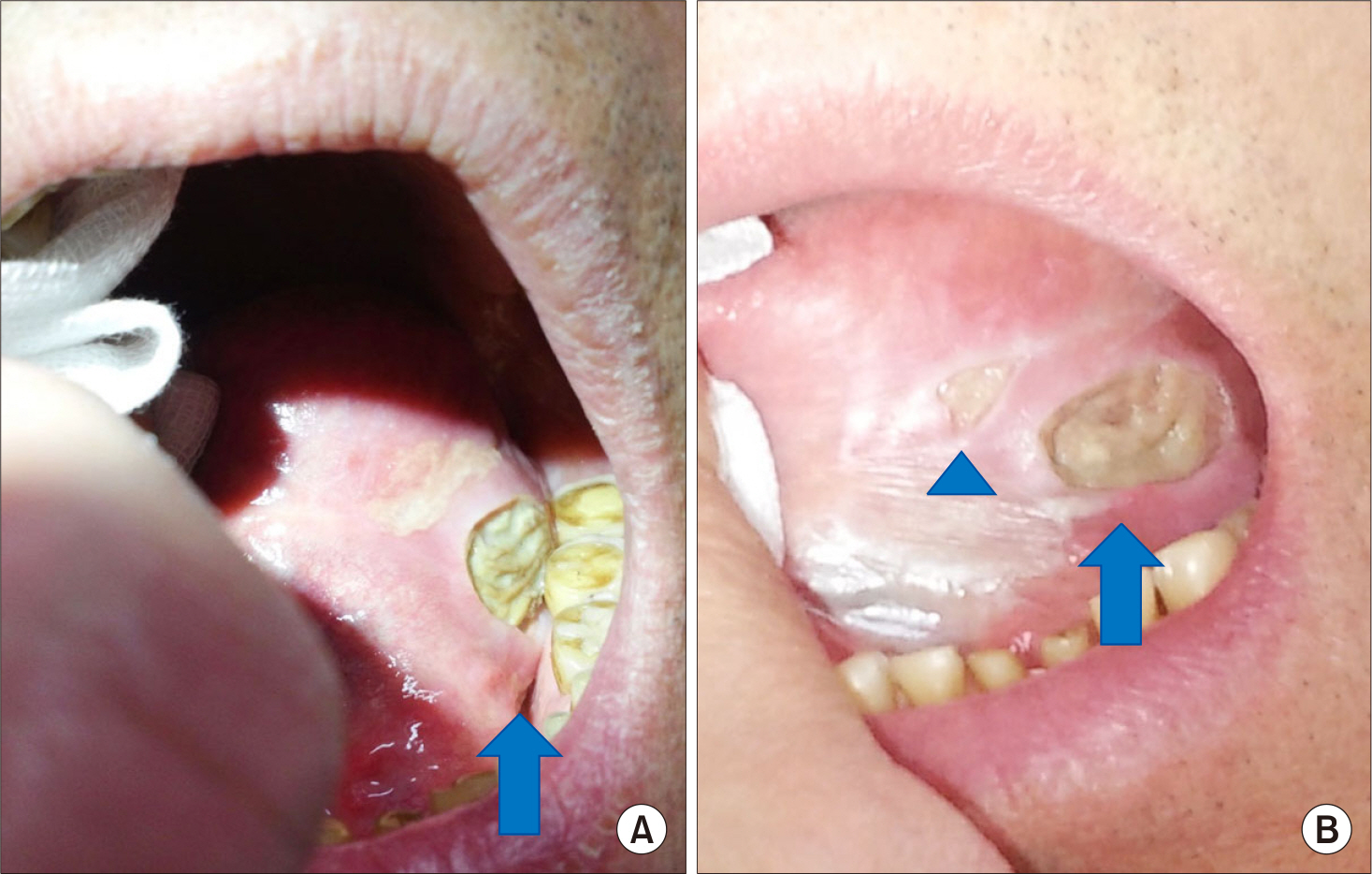
Figure 1. A 20×10 mm sized oral ulcer (arrows) with deep clean-cut margin on his left border of tongue (A), there was no any improvement but small ex-tra-ulcer (arrow head) developed during systemic steroid therapy (B).

Figure 2. Healing ulcer (arrows) at 2 months (A), and 7 months (B) from administration of adalimumab.
Reference
-
1. Field EA, Allan RB. Review article: oral ulceration– aetiopa-thogenesis, clinical diagnosis and management in the gastrointestinal clinic. Aliment Pharmacol Ther. 2003; 18:949–62.2. Beguerie JR, Sabas M. Recurrent aphthous stomatitis: an update on etiopathogenia and treatment. J Dermatol Nurses Assoc. 2015; 7:8–12.3. Altenburg A, Abdel-Naser MB, Seeber H, Abdallah M, Zouboulis CC. Practical aspects of management of recurrent aphthous stomatitis. J Eur Acad Dermatol Venereol. 2007; 21:1019–26.
Article4. Muñoz-Corcuera M, Esparza-Gómez G, González-Moles MA, Bascones-Martínez A. Oral ulcers: clinical aspects. A tool for dermatologists. Part II. Chronic ulcers. Clin Exp Dermatol. 2009; 34:456–61.
Article5. Al-Maweri SA, Ismail NM, Ismail AR, Al-Ghashm A. Prevalence of oral mucosal lesions in patients with type 2 diabetes attending hospital universiti sains malaysia. Malays J Med Sci. 2013; 20:39–46.6. Natah SS, Häyrinen-Immonen R, Hietanen J, Malmström M, Konttinen YT. Immunolocalization of tumor necrosis factor-alpha expressing cells in recurrent aphthous ulcer lesions (RAU). J Oral Pathol Med. 2000; 29:19–25.7. Hu S, Liang S, Guo H, Zhang D, Li H, Wang X, et al. Comparison of the inhibition mechanisms of adalimumab and infliximab in treating tumor necrosis factor α-associ-ated diseases from a molecular view. J Biol Chem. 2013; 288:27059–67.
Article8. Scheinfeld N. Adalimumab: a review of side effects. Expert Opin Drug Saf. 2005; 4:637–41.
Article9. Safadi RA. Prevalence of recurrent aphthous ulceration in Jordanian dental patients. BMC Oral Health. 2009; 9:31.
Article10. Vujevich J, Zirwas M. Treatment of severe, recalcitrant, major aphthous stomatitis with adalimumab. Cutis. 2005; 76:129–32.11. Sánchez-Cano D, Callejas-Rubio JL, Ruiz-Villaverde R, Ortego-Centeno N. Recalcitrant, recurrent aphthous stomatitis successfully treated with adalimumab. J Eur Acad Dermatol Venereol. 2009; 23:206.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Aphthous Stomatitis in a Healthy Adult Following COVID-19 Vaccination: Clinical Reasoning
- A Case of Intestinal Behcet's Disease Complicated Enterocutanous Fistula with a Good Response to Adalimumab
- Successful Treatment of Refractory Cutaneous Polyarteritis Nodosa with Adalimumab
- Could adalimumab be used safely and effectively in intestinal Behçet's disease refractory to conventional therapy?
- A Case of Recurrent Vogt-Koyanagi-Harada Disease Successfully Treated with Adalimumab in Young Female Adult Patient
