A Case of Intestinal Behcet's Disease Complicated Enterocutanous Fistula with a Good Response to Adalimumab
- Affiliations
-
- 1Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea. wsuhm@hanyang.co.kr
- 2Department of Rheumatology, Hanyang University Hospital for Rheumatic Disease, Seoul, Korea.
- KMID: 2223096
- DOI: http://doi.org/10.4078/jrd.2012.19.3.147
Abstract
- Behcet's disease (BD) is a multisystemic disorder, which is characterized by recurrent oral aphthous ulcers, genital ulcers, uveitis, and skin lesion. Although intestinal involvement is an uncommon manifestation of the BD, it leads to a poor prognosis, as a result of a high complication, such as intestinal perforation, fistula formation, and massive hemorrhage. Intestinal BD has the tendency for the resistance to conventional medical treatment, and it often requires a surgical intervention because of severe complication. Although the causes of intestinal BD are unknown, some studies show that tumor necrosis factor Alpha (TNF-alpha) plays a key role in the pathogenesis of BD. Therefore, anti-TNF-alpha monoclonal antibody, such as adalimumab, is one of the useful treatment for refractory and relapsed intestinal BD. We describe a patient who had intestinal BD complicated enterocutanous fistula with a good response to adalimumab.
Keyword
MeSH Terms
Figure
-
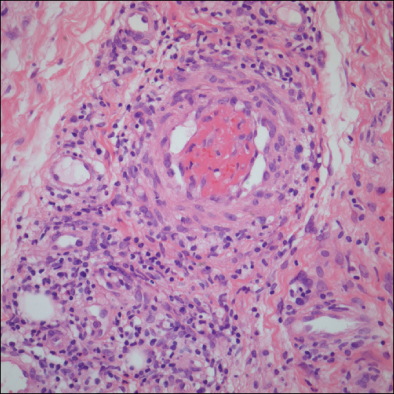
Figure 1 Skin biopsy shows mononuclear cell vasulitis with nuclear dusts and fibrioid necrosis (H&E, ×400).

Figure 2 Initial colonoscopy shows well demarcated large ulcers with a clear ulcer bed at proximal ascending colon site (A), and three month after the first adalimumab injection, follow up colonoscopy shows improvement of previous ulcers (B).

Figure 3 Colonic Biopsy shows infiltration of chronic inflammatory cell with predominant neutrophils and granulation tissue (H&E, ×400).
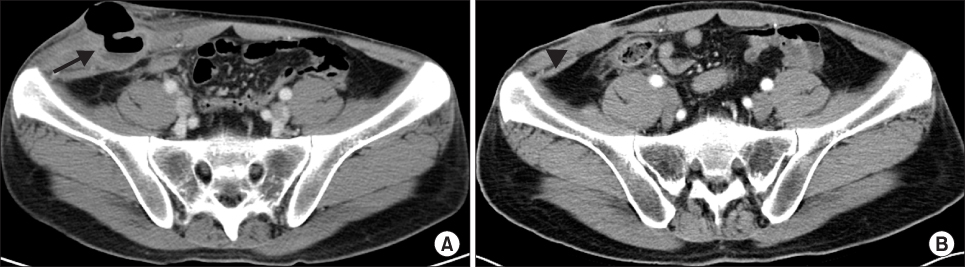
Figure 4 One month (A) after medical treatment of steroid and azathioprine and three month (B) after first administration of adalimumab, abdomen computed tomography scan shows subcutaneous abscess (arrow) with enterocutaneous fistula formation and improvement of lesions (head).
Reference
-
1. Sakane T, Takeno M, Suzuki N, Inaba G. Behçet's disease. N Engl J Med. 1999. 341:1284–1291.2. Kobayashi K, Ueno F, Bito S, Iwao Y, Fukushima T, Hiwatashi N, et al. Development of consensus statements for the diagnosis and management of intestinal Behçet's disease using a modified Delphi approach. J Gastroenterol. 2007. 42:737–745.3. Sayek I, Aran O, Uzunalimoglu B, Hersek E. Intestinal Behçet's disease: surgical experience in seven cases. Hepatogastroenterology. 1991. 38:81–83.4. Choi IJ, Kim JS, Cha SD, Jung HC, Park JG, Song IS, et al. Long-term clinical course and prognostic factors in intestinal Behçet's disease. Dis Colon Rectum. 2000. 43:692–700.5. Naganuma M, Sakuraba A, Hisamatsu T, Ochiai H, Hasegawa H, Ogata H, et al. Efficacy of infliximab for induction and maintenance of remission in intestinal Behçet's disease. Inflamm Bowel Dis. 2008. 14:1259–1264.6. Lee JH, Kim TN, Choi ST, Jang BI, Shin KC, Lee SB, et al. Remission of intestinal Behcet's disease treated with anti-tumor necrosis factor alpha monoclonal antibody (infliximab). Korean J Intern Med. 2007. 22:24–27.7. van Laar JA, Missotten T, van Daele PL, Jamnitski A, Baarsma GS, van Hagen PM. Adalimumab: a new modality for Behçet's disease? Ann Rheum Dis. 2007. 66:565–566.8. Ariyachaipanich A, Berkelhammer C, Nicola H. Intestinal Behçet's disease: maintenance of remission with adalimumab monotherapy. Inflamm Bowel Dis. 2009. 15:1769–1771.9. International Study Group for Behçet's Disease. Crieria for diagnosis of Behçet's disease. Lancet. 1990. 335:1078–1080.10. Suzuki Kurokawa M, Suzuki N. Behcet's disease. Clin Exp Med. 2004. 4:10–20.11. Cheon JH, Shin SJ, Kim SW, Lee KM, Kim JS, Kim WH. IBD Study Group of the Korean Association of the Study of Intestinal Diseases. Diagnosis of intestinal Behçet's disease. Korean J Gastroenterol. 2009. 53:187–193.12. Choi IJ, Kim JS, Park MJ, Kim YS, Lee JH, Lee DH, et al. Evaluation of prognosis and cumulative operation rate of intestinal Behcet's disease in comparison with Crohn's disease. Korean J Gastroenterol. 2000. 36:504–514.13. Misumi M, Hagiwara E, Takeno M, Takeda Y, Inoue Y, Tsuji T, et al. Cytokine production profile in patients with Behcet's disease treated with infliximab. Cytokine. 2003. 24:210–218.14. Sfikakis PP, Markomichelakis N, Alpsoy E, Assaad-Khalil S, Bodaghi B, Gul A, et al. Anti-TNF therapy in the management of Behcet's disease--review and basis for recommendations. Rheumatology (Oxford). 2007. 46:736–741.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Remission of Refractory Intestinal Behcet's Disease with Infliximab
- Switching to Etanercept in Intestinal Behcet's Disease Complicated by Secondary Non-response to Anti-TNF-alpha Antibodies
- Update on the Treatment of Intestinal Behcet's Disease
- Adalimumab or infliximab: which is better for perianal fistula in Crohn's disease?
- A Case of Spontaneous Duodenoileal Fistula in Behcet's Disease
