Rotational Alignment of the Distal Femur in Korean Female Patients with Osteoarthritis Using a Computer Image Program
- Affiliations
-
- 1Department Orthopaedic Surgery, Jeju National University Hospital, Jeju National University School of Medicine, Jeju, Korea. pyk184@hanmail.net
- KMID: 2384558
- DOI: http://doi.org/10.4055/jkoa.2017.52.3.272
Abstract
- PURPOSE
The purpose of this study was to propose a method to measurement of the exact anatomical alignment from the femur using a reference axis on computed tomography (CT) images and compare the difference of alignment axis between healthy young females and female patients with osteoarthritis of knee.
MATERIALS AND METHODS
A total of 218 female patients with osteoarthritis of the knee joint (OA group), who underwent total knee arthroplasty, between January 2013 and December 2014, were enrolled in this study. The control group included 50 female patients with healthy knee joint. Each study subjects took a CT scan of their knee, and a series of axial CT images of the distal femur were overlapped using the image program. Angles were measured among the anteroposterior (AP) axis, posterior condylar axis (PCA), anatomical transepicondylar axis (aTEA), and surgical transepicondylar axis (sTEA). The differences of rotation angle between the normal and osteoarthritic knee were evaluated.
RESULTS
The mean AP-PCA angle in the OA group was 92.9°±1.70°, whereas that in the control group was 96.3°±1.87° (p<0.01). The mean AP-aTEA angle was 84.5°±2.59°, and 90.8°±1.12° respectively (p<0.01). The mean AP-sTEA angle in the OA group was 88.7°±1.98°, whereas that in the control group was 95.1°±1.27° (p<0.01). The mean aTEA-PCA angle in the OA group was 8.4°±2.84°, while control group was 5.5°±2.00° (p<0.01). The mean sTEA-PCA angle in the OA group was 4.3°±1.17°, whereas that in the control group was 1.2°±2.10° (p=0.917).
CONCLUSION
We measured the exact relationship between the rotational axes of the distal femur by overlapping the axial images of a CT scan. The OA group revealed a more internally rotated AP axis compared with aTEA and an increased angle of aTEA-PCA than control group.
Keyword
MeSH Terms
Figure
-
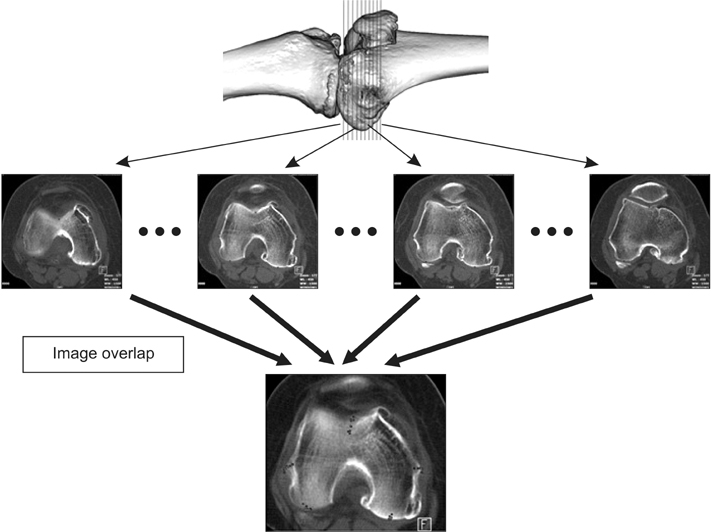
Figure 1 Reference points for each axis for all axial cuts obtained by computed tomography imaging were overlapped as one comprehensive image using a computer imaging program.
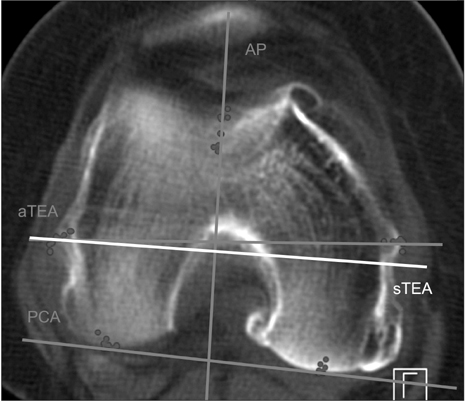
Figure 2 Computed tomography images demonstrate an axial view of the distal femoral condyle. AP, anteroposterior axis; aTEA, anatomical transepicondylar axis; sTEA, surgical transepicondylar axis; PCA, posterior condylar axis.
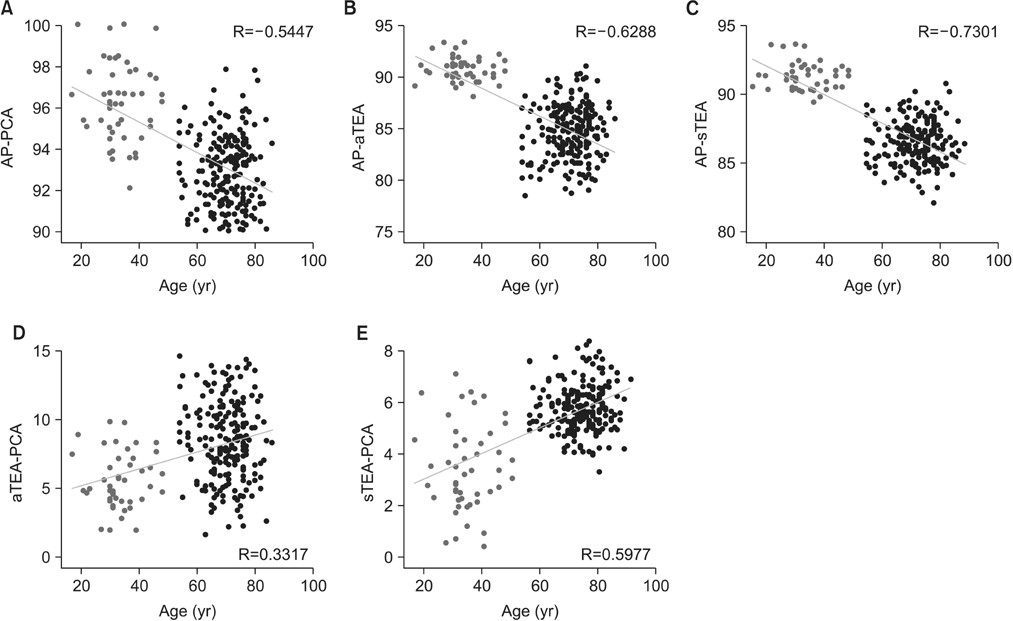
Figure 3 Correlation of the distribution of angles measured between the two axes (A: AP-PCA, B: AP-aTEA, C: AP-sTEA, D: aTEA-PCA, E: sTEA-PCA) and age (black dots: patients group, grey dots: control group). AP-PCA, anteroposterior-posterior condylar axis; AP-aTEA, anteroposterior-anatomical transepicondylar axis; AP-sTEA, anteroposterior-surgical transepicondylar axis; aTEA-PCA, anatomical transepicondylar axis-posterior condylar axis; sTEA-PCA, surgical transepicondylar axis-posterior condylar axis.

Figure 4 Correlation of the distribution of angles measured between two axes (A: AP-PCA, B: AP-aTEA, C: AP-sTEA, D: aTEA-PCA, E: sTEA-PCA) and H-K-A angle (black dots: patients group, grey dots: control group). H-K-A angle, hip-knee-ankle angle; AP-PCA, anteroposterior-posterior condylar axis; AP-aTEA, anteroposterior-anatomical transepicondylar axis; AP-sTEA, anteroposterior-surgical transepicondylar axis; aTEA-PCA, anatomical transepicondylar axis-posterior condylar axis; sTEA-PCA, surgical transepicondylar axis-posterior condylar axis.

Figure 5 The anteroposterior-anatomical transepicondylar axis (AP-aTEA) angle from axial computed tomography image of same patient showed subtle difference among the different axial level. (A) AP-aTEA angle: 5°, (B) AP-aTEA angle: 3°.
Reference
-
1. Berger RA, Rubash HE, Seel MJ, Thompson WH, Crossett LS. Determining the rotational alignment of the femoral component in total knee arthroplasty using the epicondylar axis. Clin Orthop Relat Res. 1993; (286):40–47.
Article2. Arima J, Whiteside LA, McCarthy DS, White SE. Femoral rotational alignment, based on the anteroposterior axis, in total knee arthroplasty in a valgus knee. A technical note. J Bone Joint Surg Am. 1995; 77:1331–1334.
Article3. Olcott CW, Scott RD. The Ranawat Award. Femoral component rotation during total knee arthroplasty. Clin Orthop Relat Res. 1999; (367):39–42.4. Akagi M, Matsusue Y, Mata T, et al. Effect of rotational alignment on patellar tracking in total knee arthroplasty. Clin Orthop Relat Res. 1999; (366):155–163.
Article5. Anouchi YS, Whiteside LA, Kaiser AD, Milliano MT. The effects of axial rotational alignment of the femoral component on knee stability and patellar tracking in total knee arthroplasty demonstrated on autopsy specimens. Clin Orthop Relat Res. 1993; (287):170–177.
Article6. Akagi M, Yamashita E, Nakagawa T, Asano T, Nakamura T. Relationship between frontal knee alignment and reference axes in the distal femur. Clin Orthop Relat Res. 2001; (388):147–156.
Article7. Tanavalee A, Yuktanandana P, Ngarmukos C. Surgical epicondylar axis vs anatomical epicondylar axis for rotational alignment of the femoral component in total knee arthroplasty. J Med Assoc Thai. 2001; 84:Suppl 1. S401–S408.8. Chang CB, Seong SC, Lee S, Lee MC. Anatomical assessment of the distal femur and tibia for optimal femoral rotational alignment in total knee arthroplasty. J Korean Knee Soc. 2010; 22:46–55.9. Griffin FM, Math K, Scuderi GR, Insall JN, Poilvache PL. Anatomy of the epicondyles of the distal femur: MRI analysis of normal knees. J Arthroplasty. 2000; 15:354–359.10. Yoshino N, Takai S, Ohtsuki Y, Hirasawa Y. Computed tomography measurement of the surgical and clinical transepicondylar axis of the distal femur in osteoarthritic knees. J Arthroplasty. 2001; 16:493–497.
Article11. Yoshioka Y, Siu D, Cooke TD. The anatomy and functional axes of the femur. J Bone Joint Surg Am. 1987; 69:873–880.
Article12. Blaha JD, Mancinelli CA, Simons WH, Kish VL, Thyagarajan G. Kinematics of the human knee using an open chain cadaver model. Clin Orthop Relat Res. 2003; (410):25–34.
Article13. Moreland JR, Bassett LW, Hanker GJ. Radiographic analysis of the axial alignment of the lower extremity. J Bone Joint Surg Am. 1987; 69:745–749.
Article14. Shon HC, Choi ES, Kim YM, et al. Femoral component rotation of total knee arthroplasty in Korean subjects: a study using grand piano sign and computed tomography. J Korean Orthop Assoc. 2012; 47:432–438.
Article15. Chon JG, Sun DH, Jung JY, Kim TI, Jang SW. Rotational alignment of femoral component for minimal medial collateral ligament release in total knee arthroplasty. Knee Surg Relat Res. 2011; 23:153–158.
Article16. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979; 86:420–428.
Article17. Griffin FM, Insall JN, Scuderi GR. The posterior condylar angle in osteoarthritic knees. J Arthroplasty. 1998; 13:812–815.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- MRI Measurement of the Distal Femur for Determining the Rotational Alignment in TKA
- Anatomical Assessment of Distal Femur for Optimal Femoral Component Rotational Alignment in TKA
- Regional Distribution of Stress on the Distal Femur in Advanced Osteoarthritis
- Measurement of the Axial Rotational Axis of Distal Femur Using Different Landmarks
- Anatomical Assessment of the Distal Femur and Tibia for Optimal Femoral Rotational Alignment in Total Knee Arthroplasty
