J Korean Soc Surg Hand.
2017 Jun;22(2):112-116. 10.12790/jkssh.2017.22.2.112.
Forearm Compartment Syndrome after Transradial Percutaneous Coronary Artery Intervention
- Affiliations
-
- 1Department of Orthopedic Surgery, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea. yoojoon@catholic.ac.kr
- KMID: 2383803
- DOI: http://doi.org/10.12790/jkssh.2017.22.2.112
Abstract
- Transradial percutaneous coronary artery interventions are increasingly used because of low complication rates and patients' convenience. However, the radial artery is more vulnerable to damage due to its small diameter and frequent anatomical variations. We experienced a case of forearm compartment syndrome after transradial percutaneous coronary artery intervention which has not been reported in Korean literature yet. We report the case with a review of the literature.
MeSH Terms
Figure
-
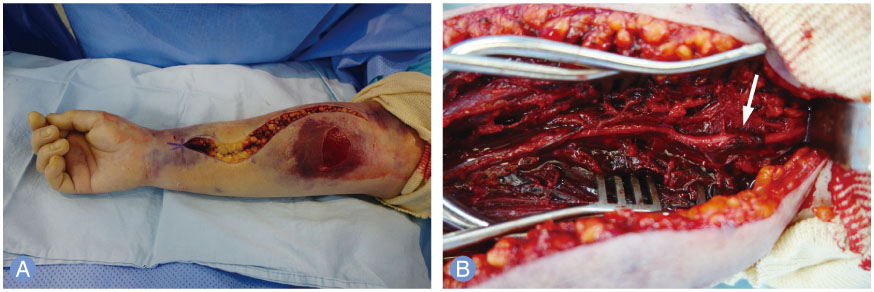
Fig. 1 (A) Intraoperative photograph showing widespread bruise and diffuse swelling of right forearm. Severe swelling and bullae formation induced by hematoma formation was seen on proximal 1/3 of the forearm. (B) Intraoperative photograph after division of the deep fascia showing infiltrating intramuscular hematoma of flexor muscles and radial artery perforation with perivascular thrombosis at the bifurcation from the brachial artery (arrow).
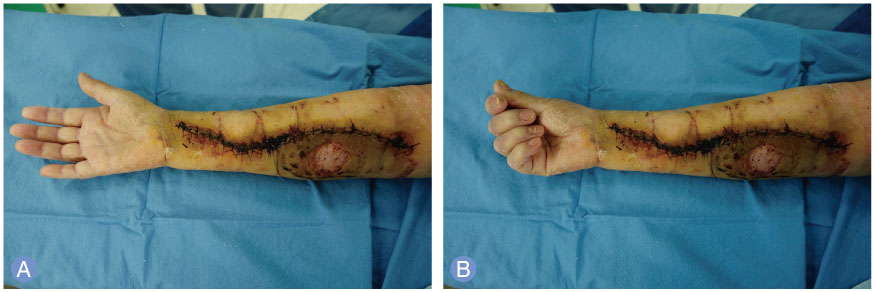
Fig. 2 Photographs taken postoperative 3 weeks showing full (A) extension and (B) flexion of all fingers.
Reference
-
1. Jolly SS, Yusuf S, Cairns J, et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011; 377:1409–1420.
Article2. Bertrand OF, Belisle P, Joyal D, et al. Comparison of transradial and femoral approaches for percutaneous coronary interventions: a systematic review and hierarchical Bayesian meta-analysis. Am Heart J. 2012; 163:632–648.
Article3. Burzotta F, Trani C, Mazzari MA, et al. Vascular complications and access crossover in 10,676 transradial percutaneous coronary procedures. Am Heart J. 2012; 163:230–238.
Article4. Dandekar VK, Vidovich MI, Shroff AR. Complications of transradial catheterization. Cardiovasc Revasc Med. 2012; 13:39–50.
Article5. Tizon-Marcos H, Barbeau GR. Incidence of compartment syndrome of the arm in a large series of transradial approach for coronary procedures. J Interv Cardiol. 2008; 21:380–384.6. Hahalis G, Tsigkas G, Kakkos S, et al. Vascular complications following transradial and transulnar coronary angiography in 1600 consecutive patients. Angiology. 2016; 67:438–443.
Article7. Yoo BS, Yoon J, Ko JY, et al. Anatomical consideration of the radial artery for transradial coronary procedures: arterial diameter, branching anomaly and vessel tortuosity. Int J Cardiol. 2005; 101:421–427.
Article8. Araki T, Itaya H, Yamamoto M. Acute compartment syndrome of the forearm that occurred after transradial intervention and was not caused by bleeding or hematoma formation. Catheter Cardiovasc Interv. 2010; 75:362–365.
Article9. Sugimoto A, Iwamoto J, Tsumuraya N, Nagaoka M, Ikari Y. Acute compartment syndrome occurring in forearm with relatively small amount of hematoma following transradial coronary intervention. Cardiovasc Interv Ther. 2016; 31:147–150.
Article10. Bertrand OF. Acute forearm muscle swelling post transradial catheterization and compartment syndrome: prevention is better than treatment. Catheter Cardiovasc Interv. 2010; 75:366–368.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Simple Management of Radial Artery Perforation during Transradial Percutaneous Coronary Intervention
- Feasibility and Problems in Transradial Coronary Angiography and Intervention
- Successful transradial intervention via a radial recurrent artery branch from the radioulnar alpha loop using a sheathless guiding catheter
- Thenar Compartment syndrome: A Case Report
- Percutaneous Transradial Approach for Coronary Angiography
