Korean J Gastroenterol.
2016 Feb;67(2):116-118. 10.4166/kjg.2016.67.2.116.
Primary Intestinal Lymphangiectasia Diagnosed by Chylous Ascites
- Affiliations
-
- 1Department of Internal Medicine, Eulji University School of Medicine, Seoul, Korea. cyk@eulji.ac.kr
- 2Department of Radiology, Eulji University School of Medicine, Seoul, Korea.
- 3Department of Pathology, Eulji University School of Medicine, Seoul, Korea.
- KMID: 2383552
- DOI: http://doi.org/10.4166/kjg.2016.67.2.116
Abstract
- No abstract available.
Figure
-

Fig. 1. Contrastenhanced abdomen CT. Nodularity of inner layer with mucosal enhancement of gastric antrum (white arrow), and ascites (black arrow) are seen.

Fig. 2. Ascites. There are gross milky color fluids obtained by paracentesis.
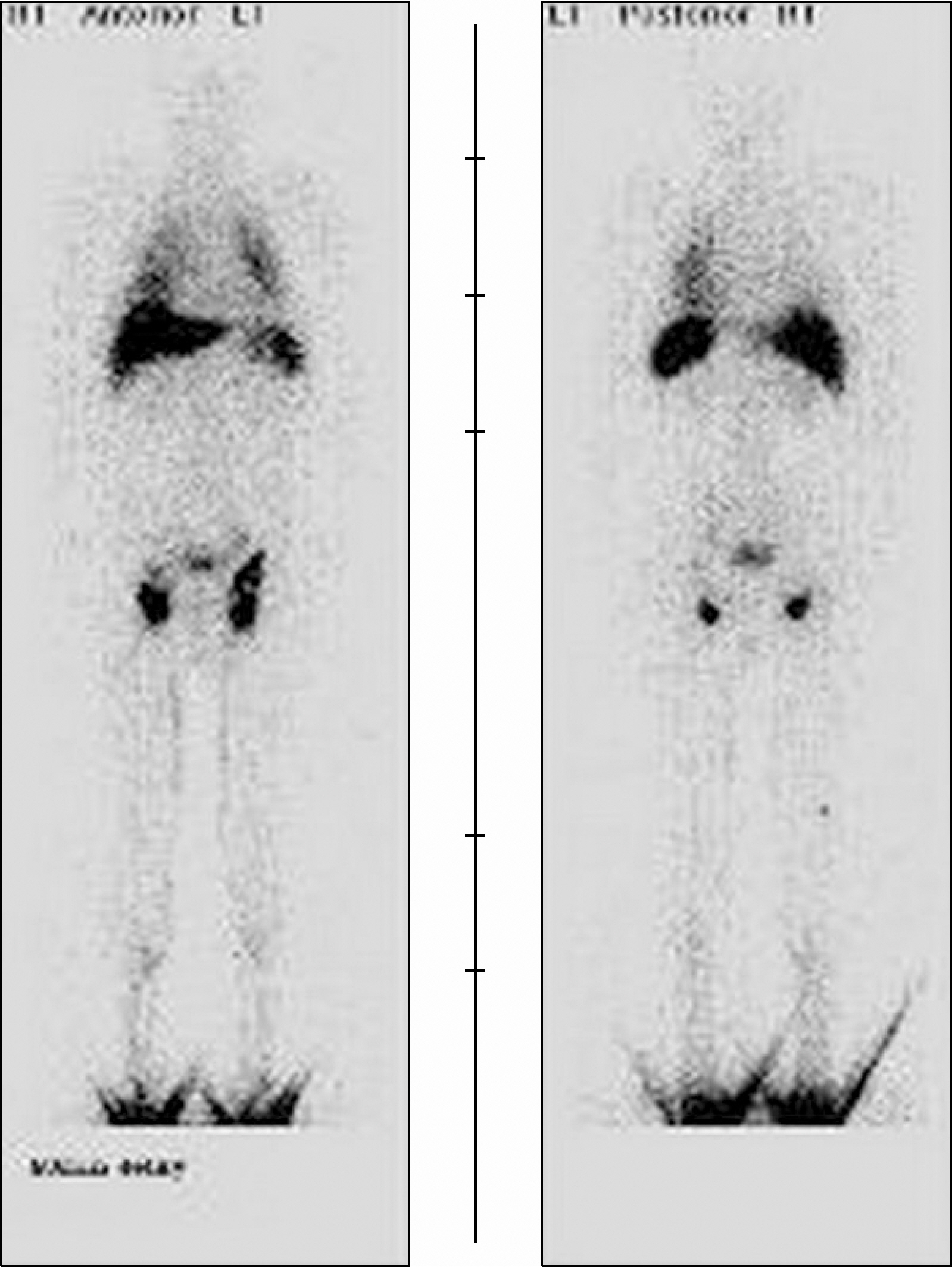
Fig. 3. Lymphangiography. There is no abrupt cut off sign or dermal back flow on lymphatic drainage.

Fig. 4. Enteroscopic findings. (A) Round elevated lesion with whitish paches. (B) After performing biopsies, white lymphatic fluid was seen flowing out from the biopsy site.
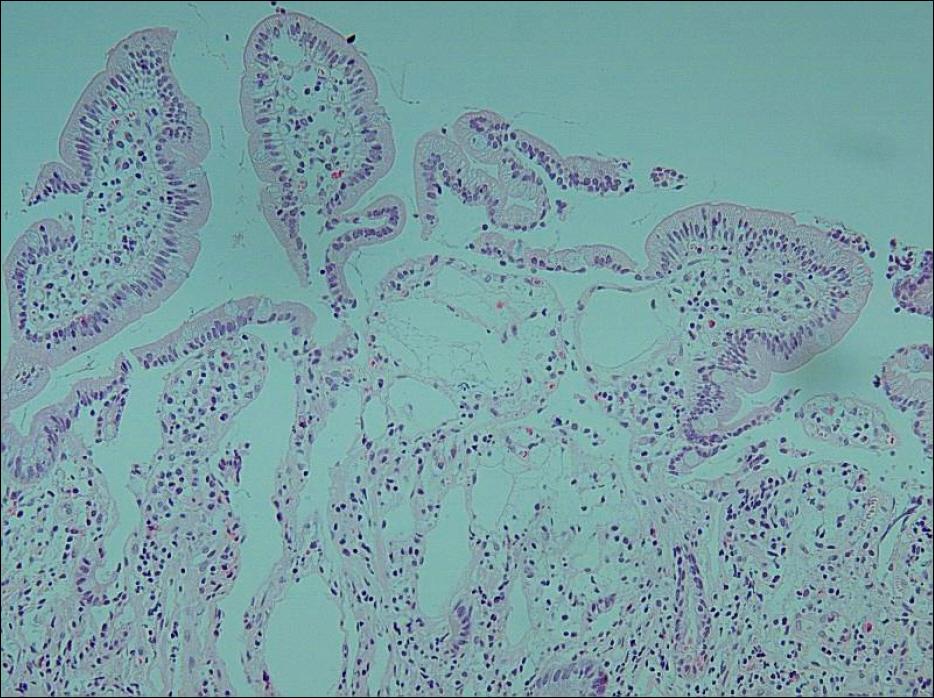
Fig. 5. Microscopic finding. The pathologic finding of proximal jejunal lesion shows dilated lymphatics containing proteinaceous fluid (H&E, ×200).
Reference
-
References
1. Wen J, Tang Q, Wu J, Wang Y, Cai W. Primary intestinal lymphangiectasia: four case reports and a review of the literature. Dig Dis Sci. 2010; 55:3466–3472.
Article2. Vignes S, Bellanger J. Primary intestinal lymphangiectasia (Waldmann's disease). Orphanet J Rare Dis. 2008; 3:5.
Article3. Umar SB, DiBaise JK. Protein-losing enteropathy: case illus-trations and clinical review. Am J Gastroenterol. 2010; 105:43–49.
Article4. Oh TG, Chung JW, Kim HM, et al. Primary intestinal lymphangiectasia diagnosed by capsule endoscopy and double balloon enteroscopy. World J Gastrointest Endosc. 2011; 3:235–240.
Article5. Rao R, Shashidhar H. Intestinal lymphangiectasia presenting as abdominal mass. Gastrointest Endosc. 2007; 65:522–523.
Article6. Maamer AB, Baazaoui J, Zaafouri H, Soualah W, Cherif A. Primary intestinal lymphangiectasia or Waldmann's disease: a rare cause of lower gastrointestinal bleeding. Arab J Gastroenterol. 2012; 13:97–98.
Article7. Imbesi V, Ciccocioppo R, Corazza GR. Long-standing intestinal lymphangiectasia detected by double-balloon enteroscopy. Clin Gastroenterol Hepatol. 2011; 9:e88–e89.
Article8. Chamouard P, Nehme-Schuster H, Simler JM, Finck G, Baumann R, Pasquali JL. Videocapsule endoscopy is useful for the diagnosis of intestinal lymphangiectasia. Dig Liver Dis. 2006; 38:699–703.
Article9. Filik L, Oguz P, Koksal A, Koklu S, Sahin B. A case with intestinal lymphangiectasia successfully treated with slow-release octreotide. Dig Liver Dis. 2004; 36:687–690.
Article10. Suehiro K, Morikage N, Murakami M, Yamashita O, Hamano K. Late-onset primary intestinal lymphangiectasia successfully managed with octreotide: a case report. Ann Vasc Dis. 2012; 5:96–99.
Article11. Zhu LH, Cai XJ, Mou YP, Zhu YP, Wang SB, Wu JG. Partial enter-ectomy: treatment for primary intestinal lymphangiectasia in four cases. Chin Med J (Engl). 2010; 123:760–764.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Idiopathic Intestinal Lymphangiectasia
- A Case of Primary Intestinal Lymphangiectasia Diagnosed by Double Balloon Enteroscopy
- The Update of Treatment for Primary Intestinal Lymphangiectasia
- A case of persistent chylous ascites after staging operation for primary fallopian tubal cancer
- Chylous Ascites Following Bariatric Surgery Report of Two Cases
