Pathology-MRI Correlation of Hepatocarcinogenesis: Recent Update
- Affiliations
-
- 1Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. medimash@gmail.com
- 2Asan Liver Center, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2381380
- DOI: http://doi.org/10.4132/jptm.2015.04.15
Abstract
- Understanding the important alterations during hepatocarcinogenesis as well as the characteristic magnetic resonance imaging (MRI) and histopathological features will be helpful for managing patients with chronic liver disease and hepatocellular carcinoma. Recent advances in MRI techniques, such as fat/iron quantification, diffusion-weighted images, and gadoxetic acid-enhanced MRI, have greatly enhanced our understanding of hepatocarcinogenesis.
Figure
-
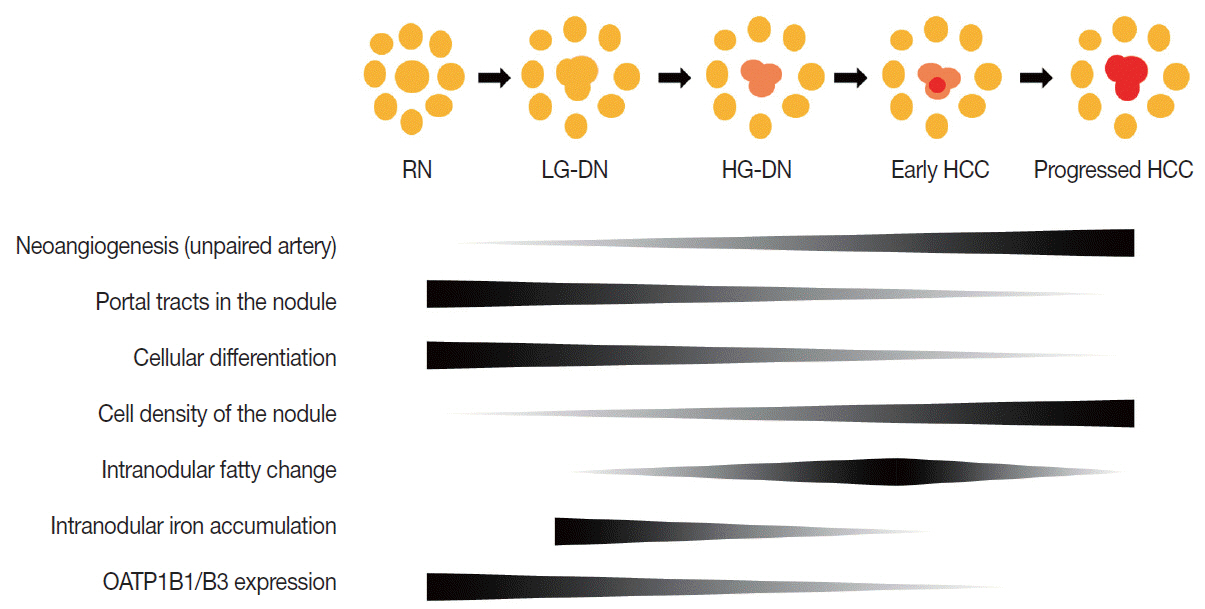
Fig. 1. Schematic view of multistep hepatocarcinogenesis. Unpaired arterial supply replaces portal supply progressively from regenerative nodules to progressed hepatocellular carcinoma (yellow, nodules with portal supply; red, nodules with unpaired arterial supply). Degrees of various pathologic components are depicted as gradient bars. DN, dysplastic nodule; HCC, hepatocellular carcinoma; HG, high grade; LG, low grade; RN, regenerative nodule.
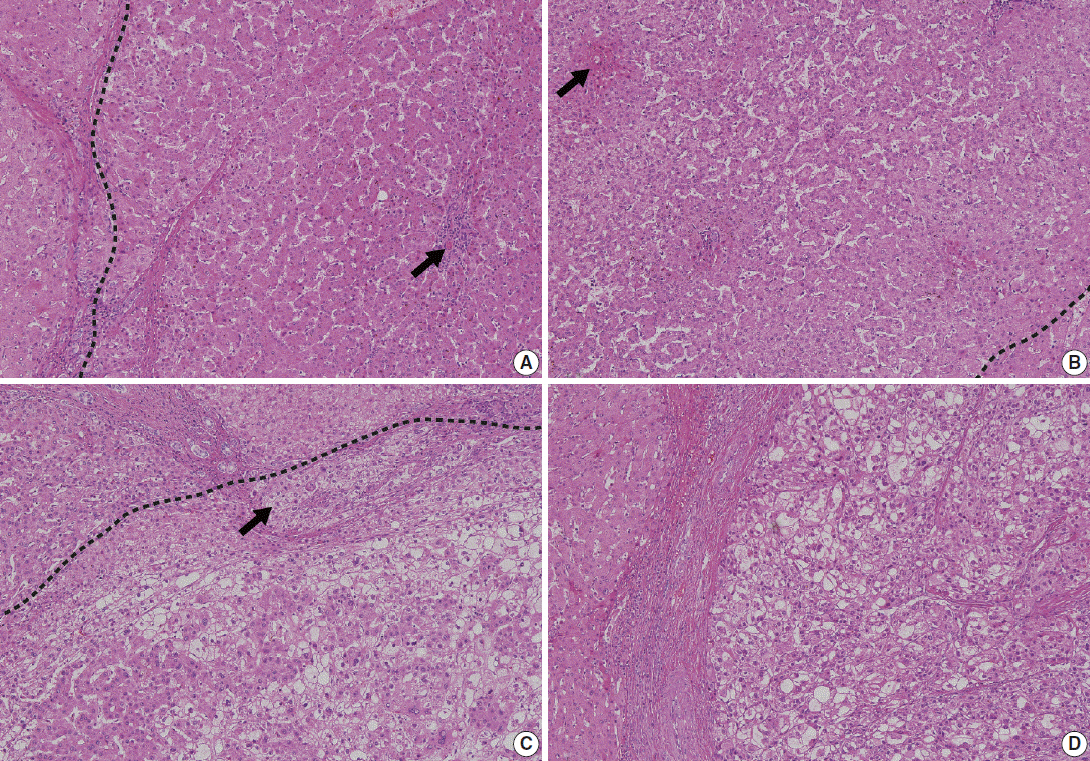
Fig. 2. Representative pathologic images of multistep hepatocarcinogenesis. (A) Low-grade dysplastic nodule (right of the dashed line) shows increased cellularity, and residual portal tracts (arrow) are easily identifiable within the nodule. (B) High-grade dysplastic nodule (left of the dashed line) shows further increased cellularity and frequent unpaired arteries (arrow). (C) Early hepatocellular carcinoma (below the dashed line) is poorly demarcated but shows unequivocal cytological atypia and stromal invasion (arrow). (D) Advanced hepatocellular carcinoma is well demarcated by a thick capsule and shows overt features of malignancy.

Fig. 3. Routine magnetic resonance imaging sequences. (A) T2-weighted imaging is helpful for the differential diagnosis of liver tumors. Hepatocellular carcinoma (HCC) usually shows intermediate high-signal intensity (arrowheads on the left), whereas hepatic cysts show bright high-signal intensity (arrow on the right). (B) In-phase and opposed-phase images provide information regarding the fat or iron content of hepatocellular nodules. The fat component of a nodule is seen as high-signal intensity on in-phase imaging (arrowhead on the left) and as low-signal intensity on opposed-phase imaging (arrow on the middle). On histology of the resected specimen, the nodule is confirmed as a fat-containing HCC. (C) Multiphasic dynamic images and hepatobiliary-phase images. After contrast injection, T1-weighted images are obtained in the arterial phase (AP), portal-venous phase (PVP), three-minute, delayed equilibrium phase (EP), and 20-minute, delayed hepatobiliary phase (HBP) to provide hemodynamic information regarding liver tumors. An HCC (arrowheads) shows typical hemodynamic features, including enhancement on AP, and washout on PVP and EP. On HBP, the HCC is seen as a hypodense mass. (D) Diffusion-weighted imaging (DWI) and the apparent diffusion coefficient (ADC) map are helpful for evaluating the cellularity of a liver tumor. HCC mostly shows high signal intensity on DWI (arrow on the left) and low signal on the ADC map (arrowheads on the right).
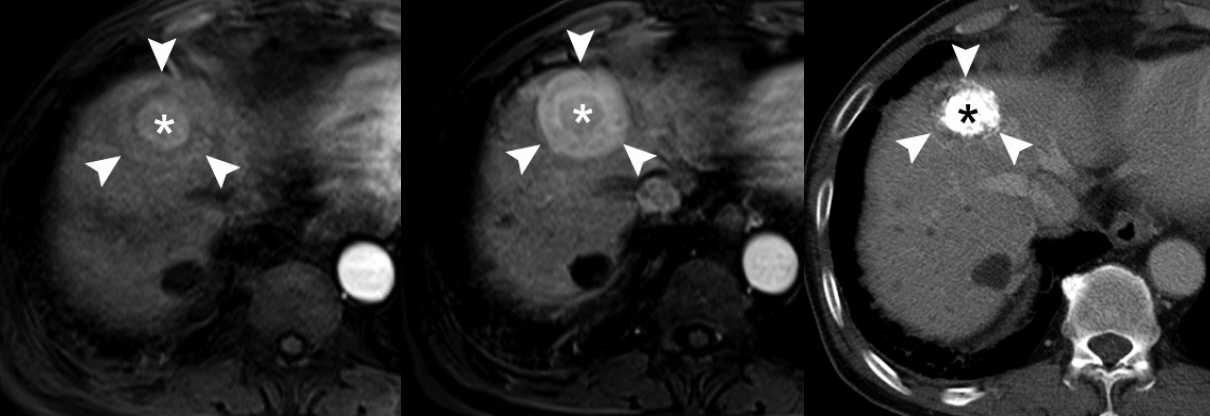
Fig. 4. Nodule-in-nodule pattern of hepatocellular carcinoma (HCC). On a multiphasic, dynamic magnetic resonance imaging of a 50-year-old patient with HCC, there is a large mass without arterial hypervascularity (arrowheads on the left) and a sub-nodule with strong arterial hypervascularity (asterisk on the left) on the arterial-phase image, i.e., the so-called nodule-in-nodule pattern. The central sub-nodule shows washout on the portal-venous phase (asterisk in the middle). After the patient was treated with transarterial chemoembolization, lipiodol was taken up only in the sub-nodule (asterisk on the right). These findings suggest the presence of HCC as a sub-nodule arising from a large dysplastic nodule.
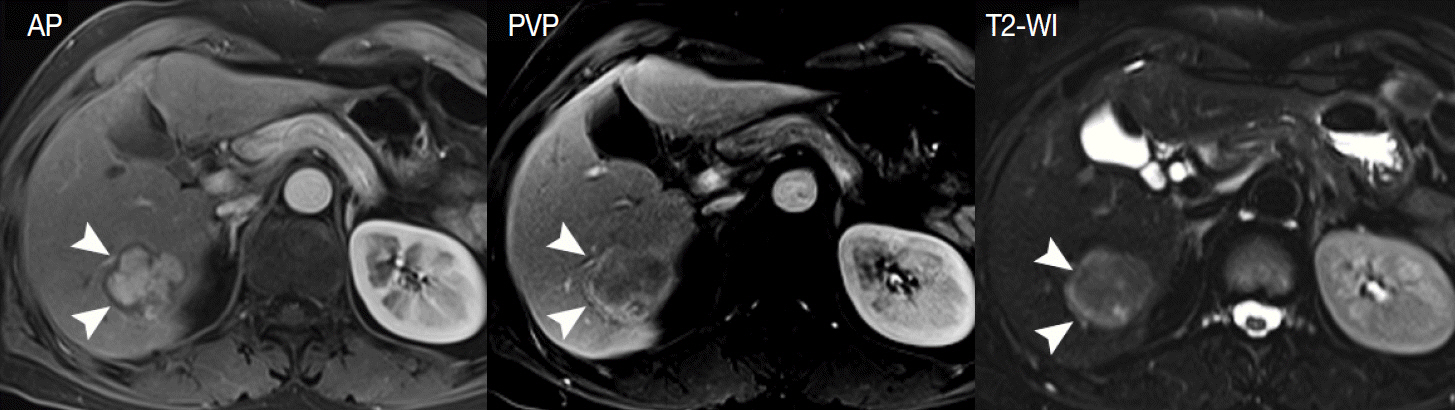
Fig. 5. Tumor capsule of the hepatocellular carcinoma (HCC). The tumor capsule (arrowheads) is seen as a hypointense rim on the arterial-phase (AP) image (left) and as an enhancing rim on the portal-venous phase (PVP) image (middle), indicating a delayed and persistent enhancement pattern. On T2-weighted imaging (T2-WI), the tumor capsule is seen as a hyperintense rim (right).

Fig. 6. Siderotic nodule. A 60-year-old patient with liver cirrhosis underwent liver magnetic resonance imaging. On in-phase images, there are many nodules with low signal intensity (arrowheads on the left), which are not clearly demonstrable on opposed-phase images (right). This signal drop of nodules on the in-phase image suggests that these nodules contain an iron component (so-called siderotic nodules).
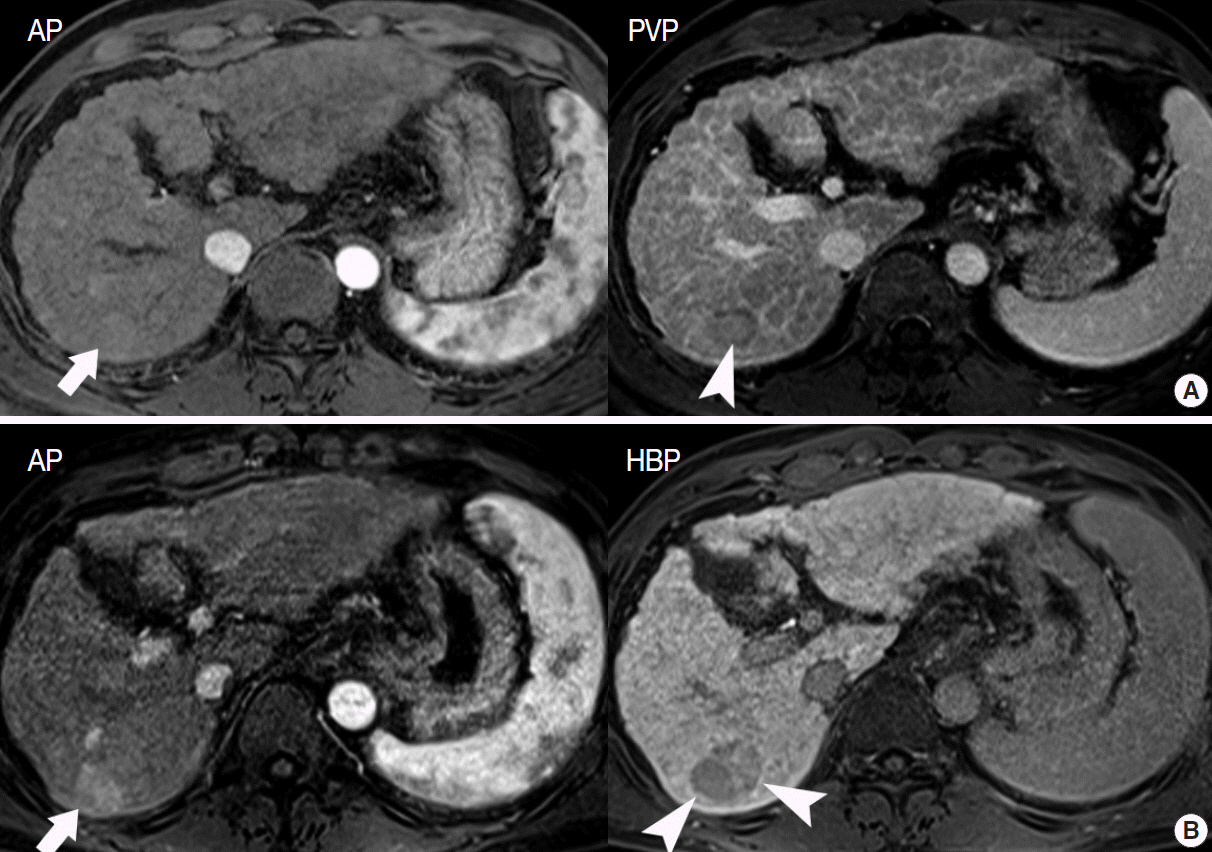
Fig. 7. A 65-year-old patient with a liver nodule. (A) On the initial magnetic resonance imaging (MRI), there is a 1.4 cm, hypointense nodule on the portal-venous phase (PVP, arrowhead) without arterial hypervascularity (arrow) on the arterial phase (AP). This nodule was regarded as a high-grade dysplastic nodule or early hepatocellular carcinoma (HCC). (B) On the one-year follow-up MRI, the nodule had increased in size. The nodule showed hypointensity on the hepatobiliary phase (HBP, arrowheads) and arterial hypervascularity on the AP (arrow), which suggests development of HCC.
Reference
-
1. Song P, Tang W, Tamura S, et al. The management of hepatocellular carcinoma in Asia: a guideline combining quantitative and qualitative evaluation. Biosci Trends. 2010; 4:283–7.2. Kudo M, Han KH, Kokudo N, et al. Liver Cancer Working Group report. Jpn J Clin Oncol. 2010; 40 Suppl 1:i19–27.
Article3. Lee SH, Choi HC, Jeong SH, et al. Hepatocellular carcinoma in older adults: clinical features, treatments, and survival. J Am Geriatr Soc. 2011; 59:241–50.
Article4. Kudo M. Multistep human hepatocarcinogenesis: correlation of imaging with pathology. J Gastroenterol. 2009; 44 Suppl 19:112–8.
Article5. Yoo HJ, Lee JM, Lee MW, et al. Hepatocellular carcinoma in cirrhotic liver: double-contrast-enhanced, high-resolution 3.0T-MR imaging with pathologic correlation. Invest Radiol. 2008; 43:538–46.
Article6. Choi BI, Lee JM. Advancement in HCC imaging: diagnosis, staging and treatment efficacy assessments: imaging diagnosis and staging of hepatocellular carcinoma. J Hepatobiliary Pancreat Sci. 2010; 17:369–73.7. Henninger B, Zoller H, Rauch S, et al. Automated two-point dixon screening for the evaluation of hepatic steatosis and siderosis: comparison with R2*-relaxometry and chemical shift-based sequences. Eur Radiol. 2015; 25:1356–65.
Article8. Suh CH, Kim KW, Kim GY, Shin YM, Kim PN, Park SH. The diagnostic value of Gd-EOB-DTPA-MRI for the diagnosis of focal nodular hyperplasia: a systematic review and meta-analysis. Eur Radiol. 2015; 25:950–60.
Article9. Krinsky G. Imaging of dysplastic nodules and small hepatocellular carcinomas: experience with explanted livers. Intervirology. 2004; 47:191–8.
Article10. Fournier LS, Cuenod CA, de Bazelaire C, et al. Early modifications of hepatic perfusion measured by functional CT in a rat model of hepatocellular carcinoma using a blood pool contrast agent. Eur Radiol. 2004; 14:2125–33.
Article11. Roncalli M, Terracciano L, Di Tommaso L, et al. Liver precancerous lesions and hepatocellular carcinoma: the histology report. Dig Liver Dis. 2011; 43 Suppl 4:S361–72.
Article12. Ishigami K, Yoshimitsu K, Nishihara Y, et al. Hepatocellular carcinoma with a pseudocapsule on gadolinium-enhanced MR images: correlation with histopathologic findings. Radiology. 2009; 250:435–43.
Article13. Kutami R, Nakashima Y, Nakashima O, Shiota K, Kojiro M. Pathomorphologic study on the mechanism of fatty change in small hepatocellular carcinoma of humans. J Hepatol. 2000; 33:282–9.
Article14. Pascale RM, De Miglio MR, Muroni MR, et al. Transferrin and transferrin receptor gene expression and iron uptake in hepatocellular carcinoma in the rat. Hepatology. 1998; 27:452–61.
Article15. Holmstrom P, Gåfvels M, Eriksson LC, et al. Expression of iron regulatory genes in a rat model of hepatocellular carcinoma. Liver Int. 2006; 26:976–85.
Article16. Libbrecht L, Craninx M, Nevens F, Desmet V, Roskams T. Predictive value of liver cell dysplasia for development of hepatocellular carcinoma in patients with non-cirrhotic and cirrhotic chronic viral hepatitis. Histopathology. 2001; 39:66–73.
Article17. Choi JY, Lee JM, Sirlin CB. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: part I. Development, growth, and spread: key pathologic and imaging aspects. Radiology. 2014; 272:635–54.
Article18. International Working Party. Terminology of nodular hepatocellular lesions. Hepatology. 1995; 22:983–93.19. International Consensus Group for Hepatocellular Neoplasia; The International Consensus Group for Hepatocellular Neoplasia. Pathologic diagnosis of early hepatocellular carcinoma: a report of the International Consensus Group for Hepatocellular Neoplasia. Hepatology. 2009; 49:658–64.20. Park YN. Update on precursor and early lesions of hepatocellular carcinomas. Arch Pathol Lab Med. 2011; 135:704–15.
Article21. Okuda K, Peters RL, Simson IW. Gross anatomic features of hepatocellular carcinoma from three disparate geographic areas: proposal of new classification. Cancer. 1984; 54:2165–73.
Article22. Korean Liver Cancer Study Group. Pathology for prediction of liver. General rules for the study of primary liver cancer. Seoul: Korean Liver Cancer Study Group;2004. p. 39–40.23. Choi BI, Lee GK, Kim ST, Han MC. Mosaic pattern of encapsulated hepatocellular carcinoma: correlation of magnetic resonance imaging and pathology. Gastrointest Radiol. 1990; 15:238–40.
Article24. Demirjian A, Peng P, Geschwind JF, et al. Infiltrating hepatocellular carcinoma: seeing the tree through the forest. J Gastrointest Surg. 2011; 15:2089–97.
Article25. Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of 100 cases among 48,900 necropsies. Cancer. 1954; 7:462–503.26. Bruix J, Sherman M; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology. 2011; 53:1020–2.
Article27. Lee JM, Choi BI. Hepatocellular nodules in liver cirrhosis: MR evaluation. Abdom Imaging. 2011; 36:282–9.
Article28. Zech CJ, Reiser MF, Herrmann KA. Imaging of hepatocellular carcinoma by computed tomography and magnetic resonance imaging: state of the art. Dig Dis. 2009; 27:114–24.
Article29. Bitar R, Leung G, Perng R, et al. MR pulse sequences: what every radiologist wants to know but is afraid to ask. Radiographics. 2006; 26:513–37.
Article30. Kang BK, Yu ES, Lee SS, et al. Hepatic fat quantification: a prospective comparison of magnetic resonance spectroscopy and analysis methods for chemical-shift gradient echo magnetic resonance imaging with histologic assessment as the reference standard. Invest Radiol. 2012; 47:368–75.31. Ayyappan AP, Jhaveri KS. CT and MRI of hepatocellular carcinoma: an update. Expert Rev Anticancer Ther. 2010; 10:507–19.
Article32. Sun HY, Lee JM, Shin CI, et al. Gadoxetic acid-enhanced magnetic resonance imaging for differentiating small hepatocellular carcinomas (< or =2 cm in diameter) from arterial enhancing pseudolesions: special emphasis on hepatobiliary phase imaging. Invest Radiol. 2010; 45:96–103.33. Taouli B, Ehman RL, Reeder SB. Advanced MRI methods for assessment of chronic liver disease. AJR Am J Roentgenol. 2009; 193:14–27.
Article34. Taouli B, Koh DM. Diffusion-weighted MR imaging of the liver. Radiology. 2010; 254:47–66.
Article35. Bartolozzi C, Battaglia V, Bozzi E. HCC diagnosis with liver-specific MRI: close to histopathology. Dig Dis. 2009; 27:125–30.36. Hayashi M, Matsui O, Ueda K, et al. Correlation between the blood supply and grade of malignancy of hepatocellular nodules associated with liver cirrhosis: evaluation by CT during intraarterial injection of contrast medium. AJR Am J Roentgenol. 1999; 172:969–76.
Article37. Choi BI. Hepatocarcinogenesis in liver cirrhosis: imaging diagnosis. J Korean Med Sci. 1998; 13:103–16.
Article38. Han JK, Eun HW, Kim SH. Radiologic findings of dysplastic nodule. Korean J Hepatol. 2008; 14:231–4.
Article39. Hanna RF, Aguirre DA, Kased N, Emery SC, Peterson MR, Sirlin CB. Cirrhosis-associated hepatocellular nodules: correlation of histopathologic and MR imaging features. Radiographics. 2008; 28:747–69.
Article40. Trevisani F, Cantarini MC, Wands JR, Bernardi M. Recent advances in the natural history of hepatocellular carcinoma. Carcinogenesis. 2008; 29:1299–305.
Article41. Aravalli RN, Cressman EN, Steer CJ. Cellular and molecular mechanisms of hepatocellular carcinoma: an update. Arch Toxicol. 2013; 87:227–47.
Article42. Thorgeirsson SS, Grisham JW. Molecular pathogenesis of human hepatocellular carcinoma. Nat Genet. 2002; 31:339–46.
Article43. Ichikawa T, Sano K, Morisaka H. Diagnosis of pathologically early HCC with EOB-MRI: experiences and current consensus. Liver Cancer. 2014; 3:97–107.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pathology of Hepatocellular Carcinoma: Recent Update
- Role of Angiogenic Factors during the Hepatocarcinogenesis
- Recent Update of Pathology of the Pancreatic Neuroendocrine Tumor
- The dual role of transforming growth factor-beta signatures in human B viral multistep hepatocarcinogenesis: early and late responsive genes
- Advances in hepatocellular carcinoma: hepatocarcinogenesis, role of exosomal noncoding RNAs, and diagnostic pathology
