Aggressive diagnosis and treatment for posterior urethral valve as an etiology for vesicoureteral reflux or urge incontinence in children
- Affiliations
-
- 1Department of Pediatric Urology, Jichi Medical University Children's Medical Center Tochigi, Shimotsuke, Japan. hnakai@jichi.ac.jp
- KMID: 2379895
- DOI: http://doi.org/10.4111/icu.2017.58.S1.S46
Abstract
- Vesicoureteral reflux (VUR) is one of the most common diseases in pediatric urology and classified into primary and secondary VUR. Although posterior urethral valve (PUV) is well known as a cause of the secondary VUR, it is controversial that minor urethral deformity recognized in voiding cystourethrography represents mild end of PUV spectrum and contributes to the secondary VUR. We have been studying for these ten years congenital urethral obstructive lesions with special attention to its urethrographic and endoscopic morphology as well as therapeutic response with transurethral incision. Our conclusion to date is that congenital obstructive lesion in the postero-membranous urethra is exclusively PUV (types 1 and 3) and that severity of obstruction depends on broad spectrum of morphological features recognized in PUV. Endoscopic diagnostic criteria for PUV are being consolidated.
MeSH Terms
Figure
-
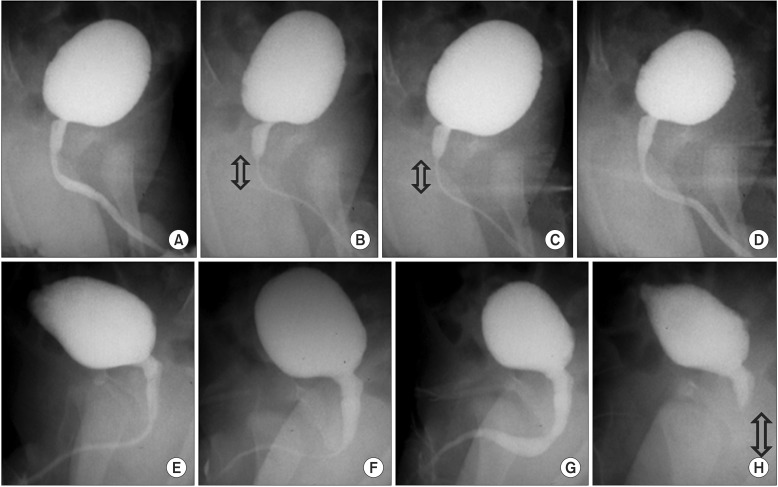
Fig. 1 In upper case (A–D), physiological discoordination (sphincteric contraction) can be seen transiently in (B) and (C) during stable urinary flow. The arrow shows area of sphincteric contraction. In bottom case (E–H), physiological discoordination occurred suddenly soon after the flow reached maximal flow rate. The arrow shows area of sphincteric contraction.
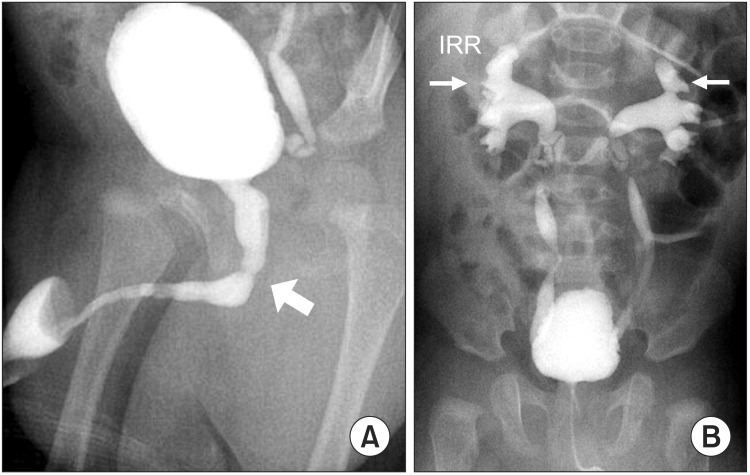
Fig. 2 (A) Overt dilatation of posterior urethra due to posterior urethral valve in 4-month old boy. The arrow depicts the location of the posterior urethral valve. (B) The same case as panel A who presented bilateral vesicoureteral reflux and IRR, resulting from high pressure voiding caused by the posterior urethral valve. IRR, intrarenal reflux.
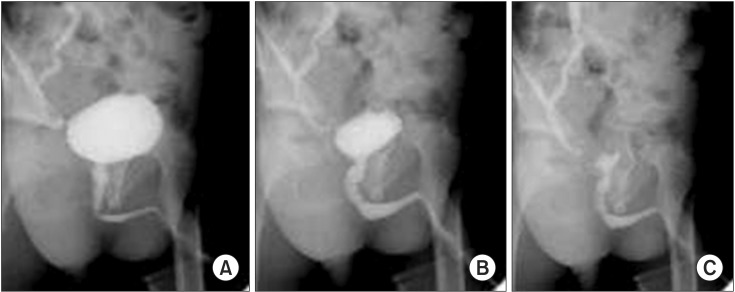
Fig. 3 Transient kinking of posterior urethra recognized in a toddler with right unilateral vesicoureteral reflux. Although the posterior urethra looked rather straight in initial voiding phase (A), it changed the shape by kinking in the mid portion of the posterior urethra (B). Finally, the kinking diminished in the terminal phase of voiding (C).
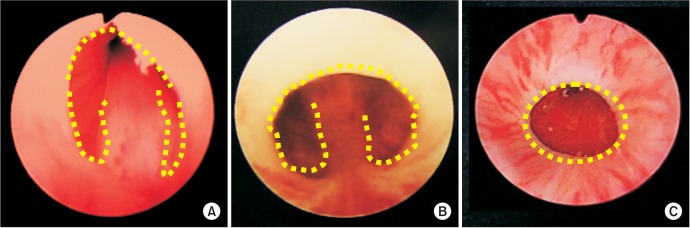
Fig. 4 Endoscopic findings of type 1 posterior urethral valves (PUVs) (A, B) and type 3 PUV (C). Valve like structure (A), membrane like structure (B), and so called “Cobb's collar” seen in type 3 PUV (C). Dotted line depicts margin of the lesion.

Fig. 5 Normal endoscopic view of membranous urethra in male children. The dotted line shows that distal part connecting to the inferior crest is flat and straight.
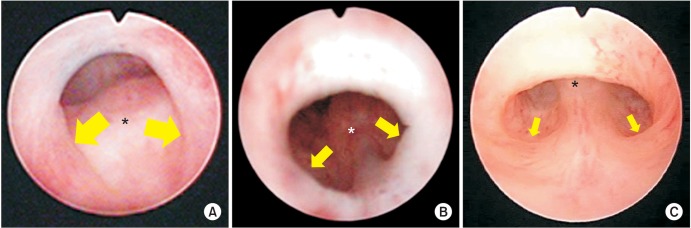
Fig. 6 Morphological spectrum of type 1 posterior urethral valve. (A) Severe type showing bilateral valve-like structure, at which cold knife is snagged deeply. (B) Moderate type showing shallow posterolateral folds. (C) Mild type showing subtle posterolateral folds. In contrast to rather thickened lesion in the anterior wall in mild to moderate types, the anterior wall lesion in severe type is thin membrane-like structure. The size of the arrows show the depth of postero-lateral folds. The asterisk indicates verumontanum. Scan this QR code to see the accompanying video, or visit www.icurology.org or https://youtu.be/xtDrhVnQhQA.
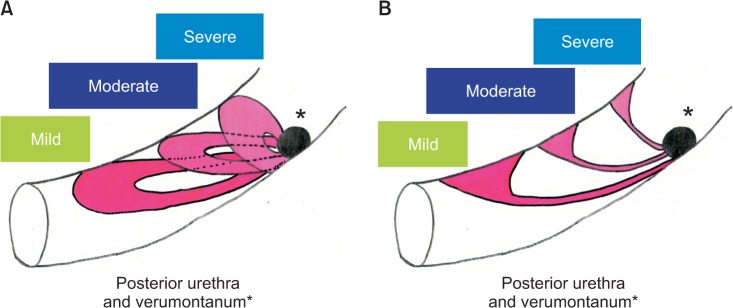
Fig. 7 (A) Lateral view of posterior urethral valve (PUV) type 1, illustrating that milder the lesion bigger the posterior defect (hole) and more distally located anterior fusion. (B) Lateral view of PUV type 1, illustrating that milder the lesion thicker the anterior lesion.
Cited by 1 articles
-
Pediatric vesicoureteral reflux: Slow but steady steps
Yong Seung Lee, Sang Won Han
Investig Clin Urol. 2017;58(Suppl 1):S1-S3. doi: 10.4111/icu.2017.58.S1.S1.
Reference
-
1. de Kort LM, Uiterwaal CS, Beek EJ, Jan Nievels RA, Klijn AJ, de Jong TP. Reliability of voiding cystourethrography to detect urethral obstruction in boys. Urology. 2004; 63:967–971. PMID: 15134990.
Article2. de Jong TP, Radmayr C, Dik P, Chrzan R, Klijn AJ, de Kort L, et al. Posterior urethral valves: search for a diagnostic reference standard. Urology. 2008; 72:1022–1025. PMID: 18585762.
Article3. Ichino M, Igawa Y, Seki S, Ishizuka O, Nishizawa O. Natural history and etiology of high pressure voiding in male infants. J Urol. 2007; 178:2561–2565. PMID: 17945306.
Article4. Dewan PA, Zappala SM, Ransley PG, Duffy PG. Endoscopic reappraisal of the morphology of congenital obstruction of the posterior urethra. Br J Urol. 1992; 70:439–444. PMID: 1450856.
Article5. Dewan PA, Keenan RJ, Morris LL, Le Quesne GW. Congenital urethral obstruction: Cobb's collar or prolapsed congenital obstructive posterior urethral membrane (COPUM). Br J Urol. 1994; 73:91–95. PMID: 8298906.
Article6. Farhat W, McLorie G, Capolicchio G, Khoury A, Bägli D, Merguerian PA. Outcomes of primary valve ablation versus urinary tract diversion in patients with posterior urethral valves. Urology. 2000; 56:653–657. PMID: 11018624.
Article7. Nakamura S, Kawai S, Kubo T, Kihara T, Mori K, Nakai H. Transurethral incision of congenital obstructive lesions in the posterior urethra in boys and its effect on urinary incontinence and urodynamic study. BJU Int. 2011; 107:1304–1311. PMID: 20804485.
Article8. Nakamura S, Hyuga T, Kawai S, Kubo T, Nakai H. The endoscopic morphological features of congenital posterior urethral obstructions in boys with refractory daytime urinary incontinence and nocturnal enuresis. Eur J Pediatr Surg. 2016; 26:368–375. PMID: 26378483.
Article9. Hyuga T, Nakamura S, Kawai S, Kubo T, Furukawa R, Aihara T, et al. The changes of urethral morphology recognized in voiding cystourethrography after endoscopic transurethral incision for posterior urethral valve in boys with intractable daytime urinary incontinence and nocturnal enuresis. World J Urol. 2017; 2. 28. [Epub]. DOI: 10.1007/s00345-017-2018-4.
Article
