Application of temporary inflow control of the Glissonean pedicle method provides a safe and easy technique for totally laparoscopic hemihepatectomy by Glissonean approach
- Affiliations
-
- 1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. chdkwon@skku.edu
- KMID: 2377712
- DOI: http://doi.org/10.4174/astr.2017.92.5.383
Abstract
- The Glissonian approach, due to its simplicity of procedure, is a technical procedure widely used in open hepatectomy. However, it is not easily applicable in the setting of the total laparoscopic approach because of movement restriction. We herein propose a new and simple method of performing hemihepatectomy by Glissonian approach called temporary inflow control of the Glissonian pedicle (TICGL) technique. Dissection of the Glisson pedicle from the liver parenchyma is done until the posterior margin of the pedicle is visualized, and is clamped with bulldog clamps. Encircling the pedicle is not necessary. Resection of the liver parenchyma is performed under inflow control of the resected side liver providing less bleeding. After sufficient resection is done so that the whole Glissonian pedicle structures are visualized, the pedicle is encircled, often very easily without the fear of bleeding from the posterior side of the pedicle, which is a common problem when encircling is done before parenchymal resection. The staplers may then be applied safely without injuring the major hepatic veins since they have been already exposed. Stapling is done while the tape is retracted toward the contralateral side. This retraction prevents injury or stricture of the contralateral Glissonian pedicle branch. The remnant liver parenchyma is resected and hepatectomy finalized. The TICGL technique provides a safe and easy way of performing major hemihepatectomies, not only by expert laparoscopic surgeons but by less experienced surgeons. It can therefore become a standard method of performing hemihepatectomy by Glissonian approach.
Keyword
MeSH Terms
Figure
-
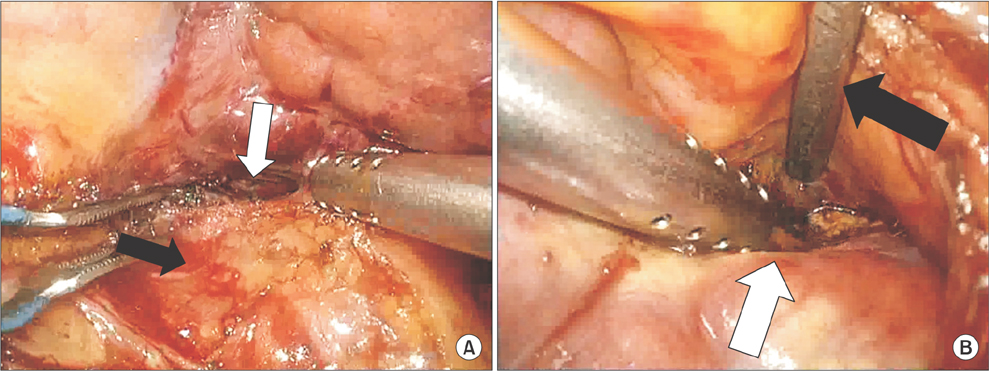
Fig. 1 The right Glissonean pedicle (black arrow) is detached from the liver surface (white arrow) by blunt dissection using bipolar clamp and suction at the superior (A) and inferior plane (B).

Fig. 2 (A) Arterial bulldog is applied on the Glissonean pedicle. (B) Additional bulldog may be applied for maximal inflow control especially in cirrhotic livers with thick pedicle. Hemostasis of minor bleeding is easily achieved with hemostatic agents.
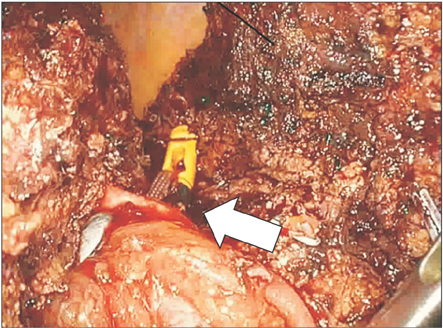
Fig. 3 After sufficient parenchymal resection is done, bifurcation of Glissonean pedicle is well exposed. A nylon tape is easily and safely encircled around the pedicle using the Goldfinger without fear of injury to the parenchyma or middle hepatic vein (white arrow).

Fig. 4 The stapling of the whole Glissonean pedicle is done. A leftward traction of the nylon tape (white arrow) during stapling enables the stapling line to be positioned sufficiently to the right side so that the left side portal vein or bile duct is not compromised making the stapling very safe.
Cited by 2 articles
-
Impact of technical innovation on surgical outcome of laparoscopic major liver resection: 10 years' experience at a large-volume center
Wontae Cho, Choon Hyuck David Kwon, Jin Yong Choi, Seung Hwan Lee, Jong Man Kim, Gyu Seong Choi, Jae-Won Joh, Sung Joo Kim, Gaab Soo Kim, Kwang Chul Koh
Ann Surg Treat Res. 2019;96(1):14-18. doi: 10.4174/astr.2019.96.1.14.Realization of improved outcomes following liver resection in hepatocellular carcinoma patients aged 75 years and older
Jong Man Kim, Jinsoo Rhu, Sang Yun Ha, Gyu-Seong Choi, Choon Hyuck David Kwon, Gaabsoo Kim, Jae-Won Joh
Ann Surg Treat Res. 2021;101(5):257-265. doi: 10.4174/astr.2021.101.5.257.
Reference
-
1. Nguyen KT, Gamblin TC, Geller DA. World review of laparoscopic liver resection-2,804 patients. Ann Surg. 2009; 250:831–841.2. Couinaud CM. A simplified method for controlled left hepatectomy. Surgery. 1985; 97:358–361.3. Takasaki K, Kobayashi S, Tanaka S. Newly developed systematized hepatectomy by Glissonean pedicle transection method. Shujutsu. 1986; 40:7–14.4. Cho A, Yamamoto H, Kainuma O, Ota T, Park S, Arimitsu H, et al. Extrahepatic Glissonean approach for laparoscopic major liver resection (with video). J Hepatobiliary Pancreat Sci. 2013; 20:141–144.5. Machado MA, Makdissi FF, Galvao FH, Machado MC. Intrahepatic Glissonian approach for laparoscopic right segmental liver resections. Am J Surg. 2008; 196:e38–e42.6. Lortat-Jacob JL, Robert HG. Well defined technic for right hepatectomy. Presse Med. 1952; 60:549–551.7. Honjo I, Araki C. Total resection of the right lobe of the liver; report of a successful case. J Int Coll Surg. 1955; 23(1 Pt 1):23–28.8. Lin TY, Chen KM, Liu TK. Total right hepatic lobectomy for primary hepatoma. Surgery. 1960; 48:1048–1060.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Application of Hepatic Resection Using Glissonean Pedicle Transection Method and Hanging Maneuver
- Impact of technical innovation on surgical outcome of laparoscopic major liver resection: 10 years' experience at a large-volume center
- Laparoscopic Liver Resection of Segments 7 and 8: from the Initial Restrictions to the Current Indications
- Intracorporeal Anastomosis in Laparoscopic Gastric Cancer Surgery
- The Feasibility of Laparoscopic Hepatectomy for the Patients with Left Intrahepatic Stones
