Breast Amyloidosis in a Female Patient with Multiple Myeloma: Ultrasonographic and Mammographic Findings
- Affiliations
-
- 1Department of Radiology, Inha University Hospital, Incheon, Korea. yalliyalla@gmail.com
- 2Department of Pathology, Inha University Hospital, Incheon, Korea.
- 3Department of Radiology, Hallym University Dongtan Sacred Heart Hospital, Hwaseong, Korea.
- KMID: 2377039
- DOI: http://doi.org/10.3348/jksr.2017.76.5.354
Abstract
- Amyloidosis is a rare disease characterized by pathological protein deposits in organs or tissues. Breast involvement by amyloidosis is rare. We report a female patient with amyloidosis in the breast, with underlying multiple myeloma, which presents as a focal asymmetry on a screening mammogram and a low suspicious mass lesion by ultrasonography.
MeSH Terms
Figure
-
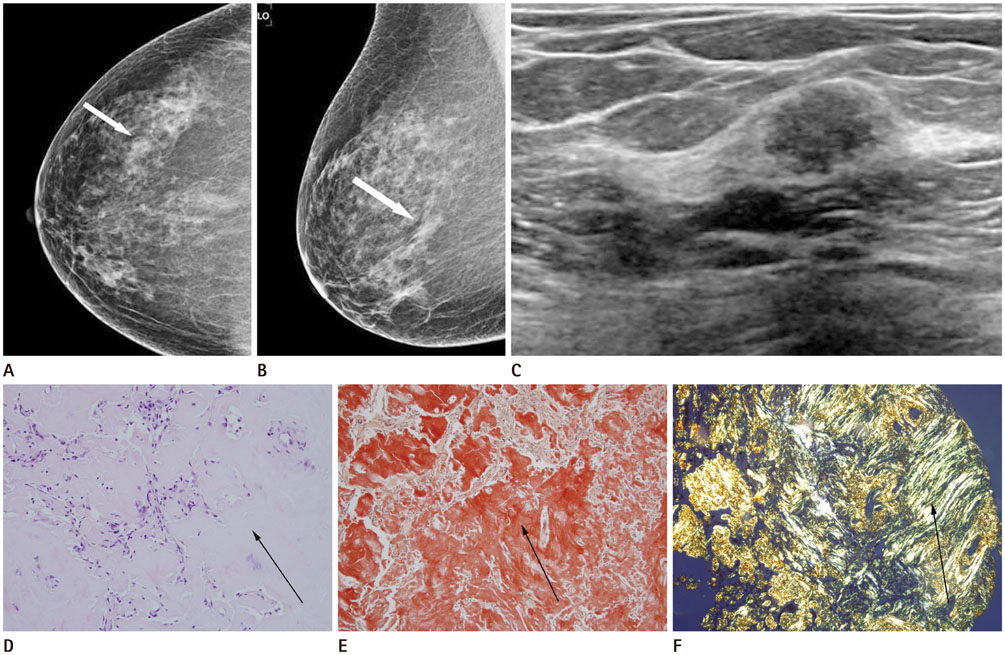
Fig. 1 Amyloidosis of the breast in a 56-year-old woman with multiple myeloma. A, B. Mammograms with craniocaudal (A) and mediolateral oblique (B) views show focal asymmetry (arrows) at the outer central portion of the right breast without microcalcification or masses. C. Ultrasonogram shows oval shaped, isoechoic mass with microlobulated margin and parallel orientation, which is located at the 9 o'clock position of the right breast and 5 cm away from the nipple (the largest diameter: 1.1 cm). D-F. Microscopic examination of 14-gauge core biopsy specimens of breast amyloidosis (D) shows amyloid deposition (arrow) in the periductal stroma of the breast. (H&E, × 200). Congo red stain (× 100) (E) reveals diffuse orange red coloring (arrow) consistent with a strong positive identification of amyloid. Polarizing microscopy (× 100) (F) reveals the characteristic apple-green birefringence (arrow) of amyloid.
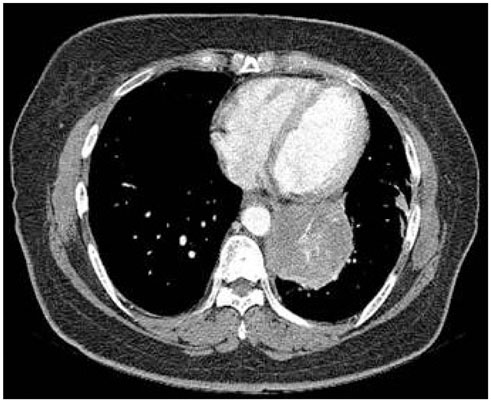
Fig. 2 Chest CT of same patient. Contrast enhanced CT scan shows an irregular enhancing mass in the left lower lung. The lesion was diagnosed as plasma cell myeloma forming amyloid tumor by surgical wedge resection.
Reference
-
1. Deolekar MV, Larsen J, Morris JA. Primary amyloid tumour of the breast: a case report. J Clin Pathol. 2002; 55:634–635.2. Said SM, Reynolds C, Jimenez RE, Chen B, Vrana JA, Theis JD, et al. Amyloidosis of the breast: predominantly AL type and over half have concurrent breast hematologic disorders. Mod Pathol. 2013; 26:232–238.3. Huerter ME, Hammadeh R, Zhou Q, Weisberg A, Riker AI. Primary amyloidosis of the breast presenting as a solitary nodule: case report and review of the literature. Ochsner J. 2014; 14:282–286.4. Fernandez BB, Hernandez FJ. Amyloid tumor of the breast. Arch Pathol. 1973; 95:102–105.5. Röcken C, Kronsbein H, Sletten K, Roessner A, Bässler R. Amyloidosis of the breast. Virchows Arch. 2002; 440:527–535.6. Sanchorawala V. Light-chain (AL) amyloidosis: diagnosis and treatment. Clin J Am Soc Nephrol. 2006; 1:1331–1341.7. Shim Y, Kim MJ, Ryu HS, Park SH. Primary breast amyloidosis presenting as microcalcifications only. Korean J Radiol. 2013; 14:723–726.8. Kumar V, Abbas AK, Aster JC. Robbins and Cotran pathologic basis of disease. 9th ed. Philadelphia: Elsevier Sciences;2014. p. 262.9. Chiang D, Lee M, Germaine P, Liao L. Amyloidosis of the breast with multicentric DCIS and pleomorphic invasive lobular carcinoma in a patient with underlying extranodal Castleman's disease. Case Rep Radiol. 2013; 2013:190856.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mammographic and Ultrasonographic Appearances of Plasmacytoma of the Breast: Case Report
- Multiple Myeloma of the Male Breast: A Case Report
- Multiple Skeletal Involvement of Multiple Myeloma Associated Amyloidosis Presented with Pathologic Fracture
- Primary Breast Amyloidosis Presenting as Microcalcifications Only
- Purpuric Bullous Skin Eruption as an Early Sign of Inconspicuous Multiple Myeloma: A Case of Amyloidosis
