Multiple Skeletal Involvement of Multiple Myeloma Associated Amyloidosis Presented with Pathologic Fracture
- Affiliations
-
- 1Department of Orthopedic Surgery, Wonju College of Medicine, Yonsei University, Wonju, Korea. chyi419@gmail.com
- KMID: 1424104
- DOI: http://doi.org/10.4055/jkoa.2013.48.2.130
Abstract
- Amyloidosis, which refers to amyloid deposits accumulated in various organs, belongs to the same category as multiple myeloma; it can be accompanied by pathologic fracture. It is important to find out the exact cause of amyloidosis in order to decide treatment options and to predict prognosis. The authors described an amyloidosis case with multiple musculoskeletal involvements presented with pathologic fracture and arthrosis, and also reviewed the related articles.
Keyword
Figure
-
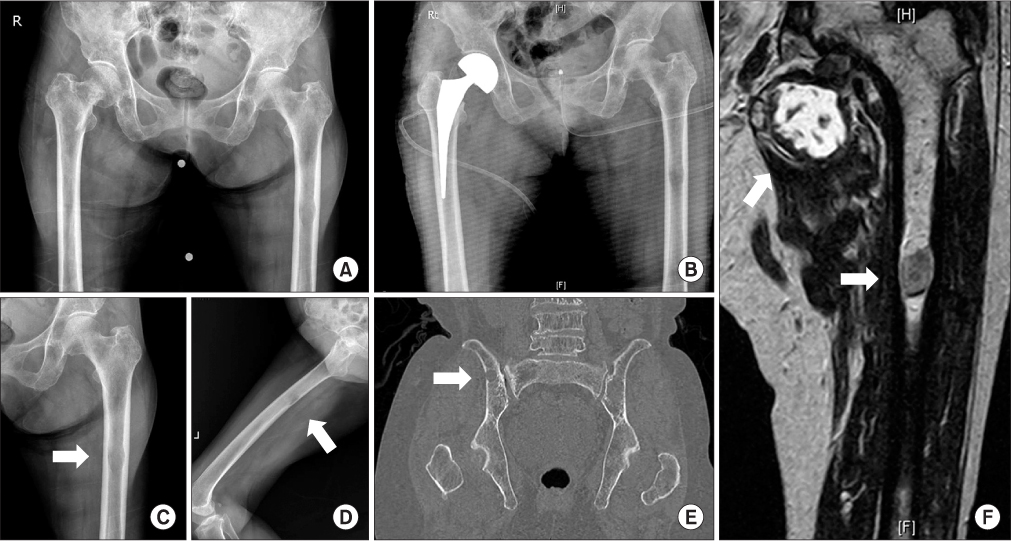
Figure 1 (A) Right femoral neck fracture was seen on the initial anterior-posterior radiograph of the pelvis. (B) Hemiarthroplasty was conducted; (C, D) however, in the left femoral shaft, an oval shaped osteolytic lesion was observed on the plain radiograph. (E) On the coronal view of pelvic computed tomography, another osteolytic lesion was seen in the right ilium. (F) On the magnetic resonance image (T1) of the left thigh, a high signal heterogenous mass was seen below the hip joint (upper arrow) and a low signal homogenous mass in the left femoral shaft.
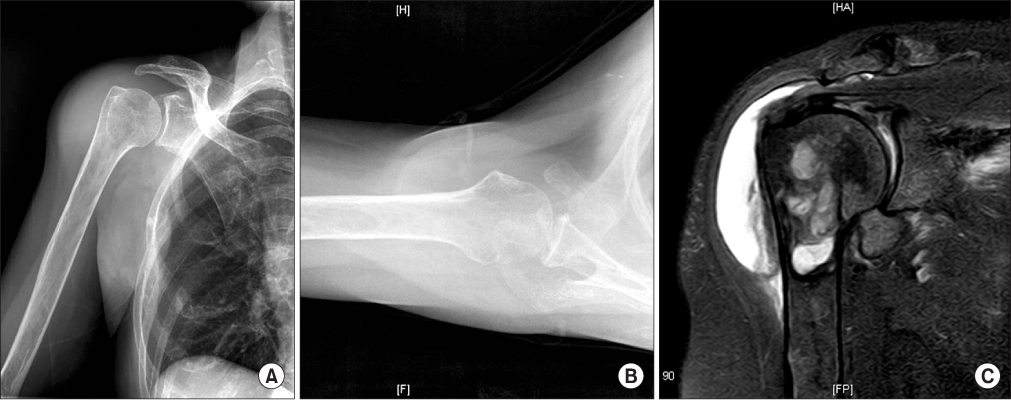
Figure 2 On the plain radiographs of the (A) antero-posterior view and (B) axial view of the shoulder, osteopenia was seen in the humeral head with diffuse swelling of the deltoid area. On the magnetic resonance image of the shoulder, fluid collection in the subdeltoid area was seen; (C) Multilobular heterogenous mass in the proximal humerus and around the soft tissue was also observed.

Figure 3 Heterogenous and less demarcated soft tissue mass mixed with bony fragment was seen in the resected mass of the humeral head as well as around the soft tissue.
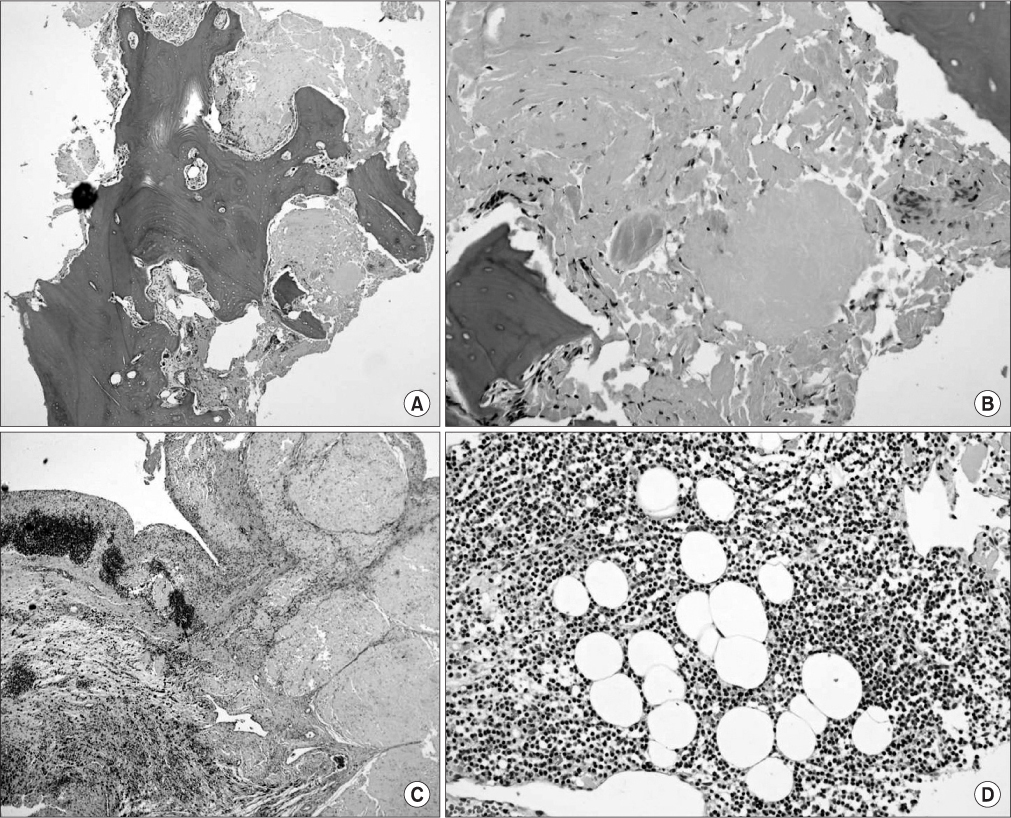
Figure 4 On H&E staining, (A) inflammatory cells and amyloid deposits were seen around the bone tissue. (C) In soft tissue mass, lobulated amyloid deposit and fibrosis with inflammatory cells were seen in the low power field (A, C: ×10 section). (B) In the high power field (B, D: ×40 section), amyloid deposit was seen significantly (D) along with plasma cell aggregation.

Figure 5 (A) In Congo red stain (×4 section), an apple-green appearance was confirmed. (B) A positive stain with light chain was seen on immunohistochemistry (×10 section).

Figure 6 (A) On urine protein electrophoresis, the monoclonal peak was seen in the kappa light chain. (B) Definite amyloid deposit was not seen in the bone marrow aspirate (H&E stain, ×10 section). (C) Diffuse plasma cell aggregation was seen (H&E stain, ×100 section). L, low; N, normal; H, high.
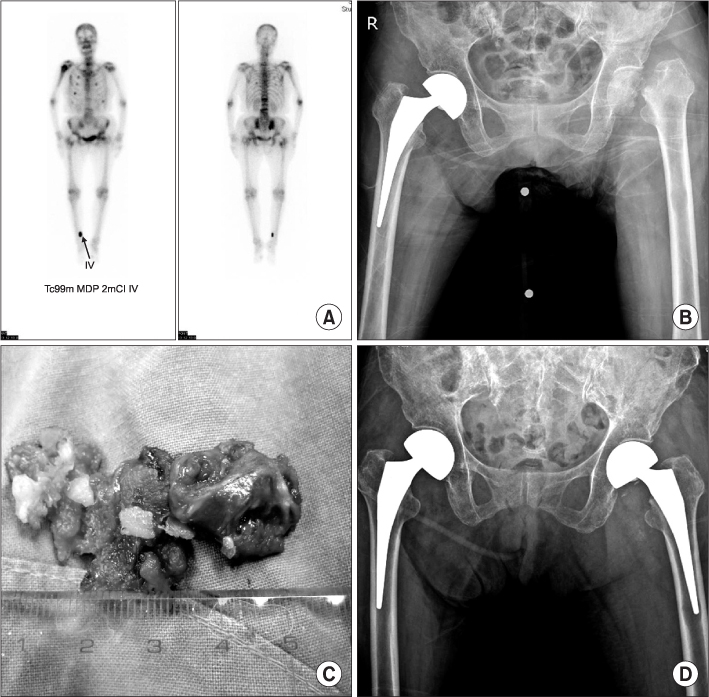
Figure 7 (A) On the bone scan, an obscure hot uptake in the left hip area was detected. (B) Femoral neck fracture with bone resorption was seen in the plain radiograph. (C) In the operative field, heterogenous, less demarcated mass with bony fragment was seen similar to shoulder mass. (D) Hemiarthroplasty was performed.
Reference
-
1. Scharschmidt TJ, Lindsey JD, Becker PS, Conrad EU. Multiple myeloma: diagnosis and orthopaedic implications. J Am Acad Orthop Surg. 2011. 19:410–419.
Article2. Fonseca R, Trendle MC, Leong T, et al. Prognostic value of serum markers of bone metabolism in untreated multiple myeloma patients. Br J Haematol. 2000. 109:24–29.
Article3. Callander NS, Roodman GD. Myeloma bone disease. Semin Hematol. 2001. 38:276–285.
Article4. Christofi T, Gupta P, Kankate L, Kankate RK. Pathological fracture of the talar neck associated with amyloid deposition. Postgrad Med J. 2007. 83:749.
Article5. Beauchamp CP. Errors and pitfalls in the diagnosis and treatment of metastatic bone disease. Orthop Clin North Am. 2000. 31:675–685.
Article6. Kyle RA, Gertz MA. Primary systemic amyloidosis: clinical and laboratory features in 474 cases. Semin Hematol. 1995. 32:45–59.7. Bahlis NJ, Lazarus HM. Multiple myeloma-associated AL amyloidosis: is a distinctive therapeutic approach warranted? Bone Marrow Transplant. 2006. 38:7–15.
Article8. Vela-Ojeda J, García-Ruiz Esparza MA, Padilla-González Y, et al. Multiple myeloma-associated amyloidosis is an independent high-risk prognostic factor. Ann Hematol. 2009. 88:59–66.
Article9. Gertz MA, Comenzo R, Falk RH, et al. Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): a consensus opinion from the 10th International Symposium on Amyloid and Amyloidosis, Tours, France, 18-22 April 2004. Am J Hematol. 2005. 79:319–328.10. Prokaeva T, Spencer B, Kaut M, et al. Soft tissue, joint, and bone manifestations of AL amyloidosis: clinical presentation, molecular features, and survival. Arthritis Rheum. 2007. 56:3858–3868.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Multiple Myeloma of Kappa Light Chain Type Associated with Gastric Amyloidosis and Acute Renal Failure and Pathologic Fracture Due to Femur Plasmacytoma
- Continuous Multiple Vertebral Compression Fractures in Multiple Myeloma Patient
- Breast Amyloidosis in a Female Patient with Multiple Myeloma: Ultrasonographic and Mammographic Findings
- Pericardial Amyloidosis Associated with Light-chain Myeloma
- A Case of Macroglossia due to Amyloidosis Associated with Multiple Myeloma
