J Gastric Cancer.
2014 Sep;14(3):187-195. 10.5230/jgc.2014.14.3.187.
Laparoscopic Distal Gastrectomy for Gastric Cancer in Morbidly Obese Patients in South Korea
- Affiliations
-
- 1Division of Gastroenterologic Surgery, Department of Surgery, Chonnam National University Hwasun Hospital, Hwasun, Korea. surgeonjeong@gmail.com
- KMID: 2372530
- DOI: http://doi.org/10.5230/jgc.2014.14.3.187
Abstract
- PURPOSE
Laparoscopic gastrectomy in obese patients has been investigated in several studies, but its feasibility has rarely been examined in morbidly obese patients, such as in those with a body mass index (BMI) of > or =30 kg/m2. The present study aimed to evaluate the technical feasibility and safety of laparoscopic gastrectomy in morbidly obese patients with gastric cancer.
MATERIALS AND METHODS
A total of 1,512 gastric cancer patients who underwent laparoscopic distal gastrectomy (LDG) were divided into three groups: normal (BMI<25 kg/m2, n=996), obese (BMI 25~30 kg/m2, n=471), and morbidly obese (BMI> or =30 kg/m2, n=45). Short-term surgical outcomes, including the course of hospitalization and postoperative complications, were compared between the three groups.
RESULTS
The morbidly obese group had a significantly longer operating time (240 minutes vs. 204 minutes, P=0.010) than the normal group, but no significant differences were found between the groups with respect to intraoperative blood loss or other complications. In the morbidly obese group, the postoperative morbidity and mortality rates were 13.3% and 0%, respectively, and the mean length of hospital stay was 8.2 days, which were not significantly different from those in the normal group. Subgroup analysis showed that postoperative complication rates were not high in morbidly obese patients, independent of the type of anastomosis technique used and level of lymph node dissection.
CONCLUSIONS
LDG is technically feasible and safe in morbidly obese patients with a BMI of > or =30 kg/m2 and early gastric carcinoma. Except for a longer operating time, LDG might represent a reasonable treatment option in these patients.
Keyword
MeSH Terms
Figure
-
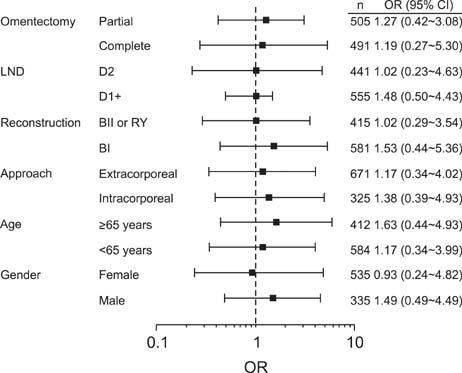
Fig. 1 Subgroup analysis for the effect of morbid obesity on the risk of postoperative complications. Morbid obesity did not increase the postoperative complications in any subgroup, regardless of the extent of lymph node dissection (LND), the types of reconstruction procedure, or the presence of omentectomy. OR = odds ratio; CI = confidence interval.
Reference
-
1. Jeong O, Park YK. Clinicopathological features and surgical treatment of gastric cancer in South Korea: the results of 2009 nationwide survey on surgically treated gastric cancer patients. J Gastric Cancer. 2011; 11:69–77.
Article2. Kim YW, Baik YH, Yun YH, Nam BH, Kim DH, Choi IJ, et al. Improved quality of life outcomes after laparoscopy-assisted distal gastrectomy for early gastric cancer: results of a prospective randomized clinical trial. Ann Surg. 2008; 248:721–727.
Article3. Memon MA, Khan S, Yunus RM, Barr R, Memon B. Meta-analysis of laparoscopic and open distal gastrectomy for gastric carcinoma. Surg Endosc. 2008; 22:1781–1789.
Article4. Viñuela EF, Gonen M, Brennan MF, Coit DG, Strong VE. Laparoscopic versus open distal gastrectomy for gastric cancer: a meta-analysis of randomized controlled trials and high-quality nonrandomized studies. Ann Surg. 2012; 255:446–456.5. Kitano S, Shiraishi N, Uyama I, Sugihara K, Tanigawa N. Japanese Laparoscopic Surgery Study GroupA multicenter study on oncologic outcome of laparoscopic gastrectomy for early cancer in Japan. Ann Surg. 2007; 245:68–72.
Article6. Lee HJ, Kim HH, Kim MC, Ryu SY, Kim W, Song KY, et al. Korean Laparoscopic Gastrointestinal Surgery Study GroupThe impact of a high body mass index on laparoscopy assisted gastrectomy for gastric cancer. Surg Endosc. 2009; 23:2473–2479.
Article7. Makino H, Kunisaki C, Izumisawa Y, Tokuhisa M, Oshima T, Nagano Y, et al. Effect of obesity on laparoscopy-assisted distal gastrectomy compared with open distal gastrectomy for gastric cancer. J Surg Oncol. 2010; 102:141–147.
Article8. Ohno T, Mochiki E, Ando H, Ogawa A, Yanai M, Toyomasu Y, et al. The benefits of laparoscopically assisted distal gastrectomy for obese patients. Surg Endosc. 2010; 24:2770–2775.
Article9. Shim JH, Song KY, Kim SN, Park CH. Laparoscopy-assisted distal gastrectomy for overweight patients in the Asian population. Surg Today. 2009; 39:481–486.
Article10. Yasuda K, Inomata M, Shiraishi N, Izumi K, Ishikawa K, Kitano S. Laparoscopy-assisted distal gastrectomy for early gastric cancer in obese and nonobese patients. Surg Endosc. 2004; 18:1253–1256.
Article11. Yamada H, Kojima K, Inokuchi M, Kawano T, Sugihara K. Effect of obesity on technical feasibility and postoperative outcomes of laparoscopy-assisted distal gastrectomy--comparison with open distal gastrectomy. J Gastrointest Surg. 2008; 12:997–1004.
Article12. Kanazawa M, Yoshiike N, Osaka T, Numba Y, Zimmet P, Inoue S. Criteria and classification of obesity in Japan and Asia-Oceania. Asia Pac J Clin Nutr. 2002; 11:Suppl 8. S732–S737.
Article13. Kim MG, Kim KC, Kim BS, Kim TH, Kim HS, Yook JH, et al. A totally laparoscopic distal gastrectomy can be an effective way of performing laparoscopic gastrectomy in obese patients (body mass index≥30). World J Surg. 2011; 35:1327–1332.
Article14. Jung MR, Park YK, Seon JW, Kim KY, Cheong O, Ryu SY. Definition and classification of complications of gastrectomy for gastric cancer based on the accordion severity grading system. World J Surg. 2012; 36:2400–2411.
Article15. Sobin LH, Gospodarowicz MK, Wittekind C, editors. TNM Classification of Malignant Tumours. 7th ed. New York: Wiley;2009.16. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011; 14:101–112.17. Dhar DK, Kubota H, Tachibana M, Kotoh T, Tabara H, Masunaga R, et al. Body mass index determines the success of lymph node dissection and predicts the outcome of gastric carcinoma patients. Oncology. 2000; 59:18–23.
Article18. Inagawa S, Adachi S, Oda T, Kawamoto T, Koike N, Fukao K. Effect of fat volume on postoperative complications and survival rate after D2 dissection for gastric cancer. Gastric Cancer. 2000; 3:141–144.
Article19. Tsujinaka T, Sasako M, Yamamoto S, Sano T, Kurokawa Y, Nashimoto A, et al. Gastric Cancer Surgery Study Group of Japan Clinical Oncology Group. Influence of overweight on surgical complications for gastric cancer: results from a randomized control trial comparing D2 and extended para-aortic D3 lymphadenectomy (JCOG9501). Ann Surg Oncol. 2007; 14:355–361.
Article20. Noshiro H, Shimizu S, Nagai E, Ohuchida K, Tanaka M. Laparoscopy-assisted distal gastrectomy for early gastric cancer: is it beneficial for patients of heavier weight? Ann Surg. 2003; 238:680–685.21. Khang YH, Yun SC. Trends in general and abdominal obesity among Korean adults: findings from 1998, 2001, 2005, and 2007 Korea National Health and Nutrition Examination Surveys. J Korean Med Sci. 2010; 25:1582–1588.
Article22. Kubo M, Sano T, Fukagawa T, Katai H, Sasako M. Increasing body mass index in Japanese patients with gastric cancer. Gastric Cancer. 2005; 8:39–41.
Article23. Kim MG, Yook JH, Kim KC, Kim TH, Kim HS, Kim BS, et al. Influence of obesity on early surgical outcomes of laparoscopic-assisted gastrectomy in gastric cancer. Surg Laparosc Endosc Percutan Tech. 2011; 21:151–154.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopic Gastrectomy and Transvaginal Specimen Extraction in a Morbidly Obese Patient with Gastric Cancer
- Corrigendum: Laparoscopic Distal Gastrectomy for Gastric Cancer in Morbidly Obese Patients in South Korea
- Laparoscopic Distal Gastrectomy for Gastric Cancer
- Intracorporeal Anastomosis in Laparoscopic Gastric Cancer Surgery
- Entirely Laparoscopic Gastrectomy and Colectomy for Remnant Gastric Cancer with Gastric Outlet Obstruction and Transverse Colon Invasion
