The Clinical Accuracy of Endoscopic Ultrasonography and White Light Imaging in Gastric Endoscopic Submucosal Dissection
- Affiliations
-
- 1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Kyungpook National University Hospital, Kyungpook National University School of Medicine, Daegu, Korea. swjeon@knu.ac.kr
Abstract
- PURPOSE
Gastric mucosal neoplastic lesions should have characteristic endoscopic features for successful endoscopic submucosal dissection.
MATERIALS AND METHODS
Out of the 1,010 endoscopic submucosal dissection, we enrolled 62 patients that had the procedure cancelled. Retrospectively, whether the reasons for cancelling the endoscopic submucosal dissection were consistent with the indications for an endoscopic submucosal dissection were assessed by analyzing the clinical outcomes of the patients that had the surgery.
RESULTS
The cases were divided into two groups; the under-diagnosed group (30 cases; unable to perform an endoscopic submucosal dissection) and the over-diagnosed group (32 cases; unnecessary to perform an endoscopic submucosal dissection), according to the second endoscopic findings, compared with the index conventional white light image. There were six cases in the under-diagnosed group with advanced gastric cancer on the second conventional white light image endoscopy, 17 cases with submucosal invasion on endoscopic ultrasonography findings, 5 cases with a size greater than 3 cm and ulcer, 1 case with diffuse infiltrative endoscopic features, and 1 case with lymph node involvement on computed tomography. A total of 25 patients underwent a gastrectomy to remove a gastric adenocarcinoma. The overall accuracy of the decision to cancel the endoscopic submucosal dissection was 40% (10/25) in the subgroup that had the surgery.
CONCLUSIONS
The accuracy of the decision to cancel the endoscopic submucosal dissection, after conventional white light image and endoscopic ultrasonography, was low in this study. Other diagnostic options are needed to arrive at an accurate decision on whether to perform a gastric endoscopic submucosal dissection.
MeSH Terms
Figure
-
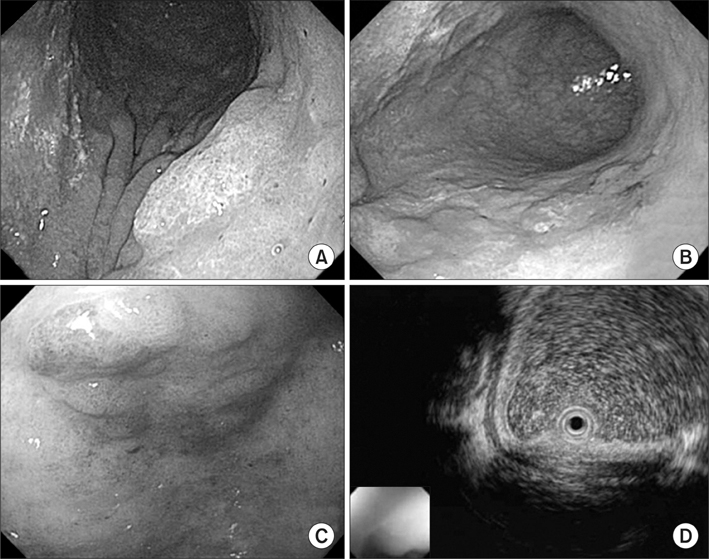
Fig. 1 Two centimeter elevated mucosal lesion was revealed as HGD on the initial diagnosis of a 63-year-old male (A). However, ulceration and a size over 3 cm were observed on the second cWLI 59 days later (B), therefore surgical treatment was performed. EGC was diagnosed on a 3 cm IIa lesion of the antrum in a 75-year-old female (C). However, the lesion already involved over 1/3 of the upper submucosa on the EUS performed 9 days later compared to the initial endoscopy (D). HGD = high grade dysplasia; cWLI = conventional white light image; EGC = early gastric cancer; EUS = endoscopic ultrasonography.

Fig. 2 Clinical outcomes of cancelled ESD cases. Among the 62 cancelled cases, 30 (19 adenocarcinoma, 5 HGD, 5 LGD, 1 atypical cell in initial diagnosis) were under-diagnosed when referred, and included six cases of gross AGC by endoscopic features, 17 cases with submucosal invasion on EUS findings, five cases over 3 cm with ulceration, one case with diffuse infiltrative endoscopic features and one case of lymph node involvement on CT. Twenty-five among the 30 under-diagnosed cases underwent subtotal gastrectomy and none had lymph node involvement. Thirty-two patients were over-diagnosed (1 atypical cell, 1 HGD, 30 LGD in initial diagnosis) and their pathology at the time of the second endoscopy was: 1 adenocarcinoma, 16 adenomas, 11 with chronic gastritis, and four cases with no suspected mucosal lesion for re-biopsy at the second endoscopy. Adenocarcinoma found in re-biopsied cases had ESD later and there were three cases that underwent ESD later with adenomas. ESD = endoscopic submucosal dissection; Adenoca = adenocarcinoma; HGD = high grade dysplasia; LGD = low grade dysplasia; AGC = advanced gastric cancer; EUS = endoscopic ultrasonography; LN = lymph node; CT = computed tomography; F/u = follow-up.
Reference
-
1. Parkin DM, Bray FI, Devesa SS. Cancer burden in the year 2000. The global picture. Eur J Cancer. 2001. 37:Suppl 8. S4–S66.
Article2. Nam SY, Choi IJ, Park KW, Kim CG, Lee JY, Kook MC, et al. Effect of repeated endoscopic screening on the incidence and treatment of gastric cancer in health screenees. Eur J Gastroenterol Hepatol. 2009. 21:855–860.
Article3. Soetikno RM, Gotoda T, Nakanishi Y, Soehendra N. Endoscopic mucosal resection. Gastrointest Endosc. 2003. 57:567–579.
Article4. Muto M, Miyamoto S, Hosokawa A, Doi T, Ohtsu A, Yoshida S, et al. Endoscopic mucosal resection in the stomach using the insulated-tip needle-knife. Endoscopy. 2005. 37:178–182.
Article5. Oka S, Tanaka S, Kaneko I, Mouri R, Hirata M, Kawamura T, et al. Advantage of endoscopic submucosal dissection compared with EMR for early gastric cancer. Gastrointest Endosc. 2006. 64:877–883.
Article6. Gotoda T, Yamamoto H, Soetikno RM. Endoscopic submucosal dissection of early gastric cancer. J Gastroenterol. 2006. 41:929–942.
Article7. Cao Y, Liao C, Tan A, Gao Y, Mo Z, Gao F. Meta-analysis of endoscopic submucosal dissection versus endoscopic mucosal resection for tumors of the gastrointestinal tract. Endoscopy. 2009. 41:751–757.
Article8. Nakamoto S, Sakai Y, Kasanuki J, Kondo F, Ooka Y, Kato K, et al. Indications for the use of endoscopic mucosal resection for early gastric cancer in Japan: a comparative study with endoscopic submucosal dissection. Endoscopy. 2009. 41:746–750.
Article9. Yamada H, Ikegami M, Shimoda T, Takagi N, Maruyama M. Long-term follow-up study of gastric adenoma/dysplasia. Endoscopy. 2004. 36:390–396.
Article10. Kim YJ, Park JC, Kim JH, Shin SK, Lee SK, Lee YC, et al. Histologic diagnosis based on forceps biopsy is not adequate for determining endoscopic treatment of gastric adenomatous lesions. Endoscopy. 2010. 42:620–626.
Article11. Gotoda T, Yanagisawa A, Sasako M, Ono H, Nakanishi Y, Shimoda T, et al. Incidence of lymph node metastasis from early gastric cancer: estimation with a large number of cases at two large centers. Gastric Cancer. 2000. 3:219–225.
Article12. Kwee RM, Kwee TC. The accuracy of endoscopic ultrasonography in differentiating mucosal from deeper gastric cancer. Am J Gastroenterol. 2008. 103:1801–1809.
Article13. Ichikawa T, Kudo M, Matsui S, Okada M, Kitano M. Endoscopic ultrasonography with three miniature probes of different frequency is an accurate diagnostic tool for endoscopic submucosal dissection. Hepatogastroenterology. 2007. 54:325–328.14. Puli SR, Batapati Krishna Reddy J, Bechtold ML, Antillon MR, Ibdah JA. How good is endoscopic ultrasound for TNM staging of gastric cancers? A meta-analysis and systematic review. World J Gastroenterol. 2008. 14:4011–4019.
Article15. Kwee RM, Kwee TC. Imaging in local staging of gastric cancer: a systematic review. J Clin Oncol. 2007. 25:2107–2116.
Article16. Kim JH, Song KS, Youn YH, Lee YC, Cheon JH, Song SY, et al. Clinicopathologic factors influence accurate endosonographic assessment for early gastric cancer. Gastrointest Endosc. 2007. 66:901–908.
Article17. Hizawa K, Iwai K, Esaki M, Matsumoto T, Suekane H, Iida M. Is endoscopic ultrasonography indispensable in assessing the appropriateness of endoscopic resection for gastric cancer? Endoscopy. 2002. 34:973–978.
Article18. Choi J, Kim SG, Im JP, Kim JS, Jung HC, Song IS. Comparison of endoscopic ultrasonography and conventional endoscopy for prediction of depth of tumor invasion in early gastric cancer. Endoscopy. 2010. 42:705–713.
Article19. Kida M, Tanabe S, Watanabe M, Kokutou M, Kondou I, Yamada Y, et al. Staging of gastric cancer with endoscopic ultrasonography and endoscopic mucosal resection. Endoscopy. 1998. 30:Suppl 1. A64–A68.
Article20. Nomura N, Goto H, Niwa Y, Arisawa T, Hirooka Y, Hayakawa T. Usefulness of contrast-enhanced EUS in the diagnosis of upper GI tract diseases. Gastrointest Endosc. 1999. 50:555–560.
Article21. Kida M, Kikuchi H, Ikeda H, Miyazawa S, Iwai T, Araki M, et al. Diagnostic of gastric cancer invasion with three-dimensional endoscopic ultrasonography, especially in cases with "SM1" invasion. Stomach Intest. 2007. 42:88–98.22. Di Gregorio C, Morandi P, Fante R, De Gaetani C. Gastric dysplasia. A follow-up study. Am J Gastroenterol. 1993. 88:1714–1719.23. Gono K, Yamazaki K, Doguchi N, Nonami T, Obi T, Yamaguchi M, et al. Endoscopic observation of tissue by narrow band illumination. Opt Rev. 2003. 10:211–215.
Article24. Nakayoshi T, Tajiri H, Matsuda K, Kaise M, Ikegami M, Sasaki H. Magnifying endoscopy combined with narrow band imaging system for early gastric cancer: correlation of vascular pattern with histopathology (including video). Endoscopy. 2004. 36:1080–1084.
Article25. Sumiyama K, Kaise M, Nakayoshi T, Kato M, Mashiko T, Uchiyama Y, et al. Combined use of a magnifying endoscope with a narrow band imaging system and a multibending endoscope for en bloc EMR of early stage gastric cancer. Gastrointest Endosc. 2004. 60:79–84.
Article26. Kadowaki S, Tanaka K, Toyoda H, Kosaka R, Imoto I, Hamada Y, et al. Ease of early gastric cancer demarcation recognition: a comparison of four magnifying endoscopy methods. J Gastroenterol Hepatol. 2009. 24:1625–1630.
Article27. Ohkawa A, Miwa H, Namihisa A, Kobayashi O, Nakaniwa N, Ohkusa T, et al. Diagnostic performance of light-induced fluorescence endoscopy for gastric neoplasms. Endoscopy. 2004. 36:515–521.
Article28. Uedo N, Iishi H, Tatsuta M, Yamada T, Ogiyama H, Imanaka K, et al. A novel videoendoscopy system by using autofluorescence and reflectance imaging for diagnosis of esophagogastric cancers. Gastrointest Endosc. 2005. 62:521–528.
Article29. Bhunchet E, Shibata T. Proposal for two strategies to prevent remnants of gastric cancers after endoscopic mucosal resections: fluorescein electronic endoscopy and rapid stump diagnosis based on pit patterns. Gastric Cancer. 2004. 7:221–232.
Article30. Haringsma J, Tytgat GN, Yano H, Iishi H, Tatsuta M, Ogihara T, et al. Autofluorescence endoscopy: feasibility of detection of GI neoplasms unapparent to white light endoscopy with an evolving technology. Gastrointest Endosc. 2001. 53:642–650.
Article31. Bhunchet E, Hatakawa H, Sakai Y, Shibata T. Fluorescein electronic endoscopy: a novel method for detection of early stage gastric cancer not evident to routine endoscopy. Gastrointest Endosc. 2002. 55:562–571.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent advances in endoscopic diagnosis and treatment of gastric cancer
- History and Development of Accessories for Endoscopic Submucosal Dissection
- Treatment of Early Gastric Cancer: Endoscopic Submucosal Dissection with LASER
- Clinical Usefulness of Dual Red Imaging in Gastric Endoscopic Submucosal Dissection: A Pilot Study
- Endoscopic Treatment for Early Gastric Cancer
