J Gastric Cancer.
2011 Dec;11(4):206-211.
Totally Laparoscopic Total Gastrectomy Using Intracorporeally Hand-Sewn Esophagojejunostomy
- Affiliations
-
- 1Department of Surgery, National Medical Center, Seoul, Korea. jmparkgs@gmail.com
Abstract
- PURPOSE
Laparoscopic total gastrectomy (LTG) for gastric cancer is still uncommon because of technical difficulties, especially in esophagojejunostomy (EJ). There are many reports for various laparoscopic procedures of EJ using linear or circular staplers. On the other hands, there has been no report for hand-sewn anastomosis. We report successfully performed intracorporeally hand-sewn EJ after LTG.
MATERIALS AND METHODS
The clinicopathologic data and short-term surgical outcomes of 6 patients who underwent totally laparoscopic total gastrectomy for upper gastric cancer from December 2010 and July 2011 were retrospectively reviewed.
RESULTS
The mean age was 66.5 years and mean body mass index (kg/m2) was 24.6. All patients had medical comorbidities. The mean patient ASA score was 2.17. Among the 6 patients, previous abdominal operation was performed for 2 patients and combined operation was performed for 3 patients. The mean blood loss, operation time, and EJ anastomosis time was 130 ml, 379.7 minutes, and 81.5 minutes, respectively. The mean time to first flatus, first oral intake, and postoperative hospital stay was 3.0, 3.0, and 12.5 days, respectively. There was no 30-day mortality case. Postoperative aspiration pneumonia and multiple periventricular lacunar infarctions developed in 1 patient. There were no anastomosis-related complications and other major surgical complications.
CONCLUSIONS
When the intracorporeal anastomotic technique becomes popular in LTG the intracorporeally hand-sewn EJ may be accepted as one method among the various laparoscopic procedures of EJ.
MeSH Terms
Figure
-
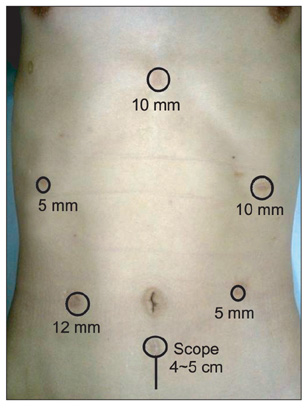
Fig. 1 Port placement and minilaparotomy for specimen removal.
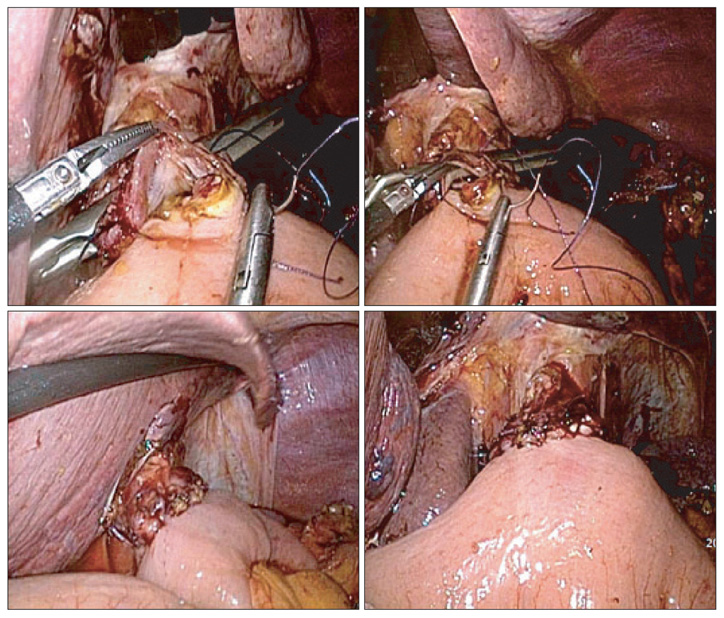
Fig. 2 Laparoscopic view for intracorporeally hand-sewn esophagojejunostomy.

Fig. 3 Postoperative contrast study and esophagogastroduodenoscopy of the first patient. (A) Constrast study was performed on postoperative day 3. It shows no anastomotic leakage. (B) It is endoscopic finding of the esophagojejunostomy site on postoperative 6 months. *It shows no anastomotic stenosis.
Reference
-
1. Azagra JS, Goergen M, De Simone P, Ibanez-Aguirre J. The current role of laparoscopic surgery in the treatment of benign gastroduodenal diseases. Hepatogastroenterology. 1999. 46:1522–1526.2. Adachi Y, Suematsu T, Shiraishi N, Katsuta T, Morimoto A, Kitano S, et al. Quality of life after laparoscopy-assisted Billroth I gastrectomy. Ann Surg. 1999. 229:49–54.
Article3. Kim MC, Kim KH, Kim HH, Jung GJ. Comparison of laparoscopy-assisted by conventional open distal gastrectomy and extraperigastric lymph node dissection in early gastric cancer. J Surg Oncol. 2005. 91:90–94.
Article4. Kitano S, Shiraishi N, Uyama I, Sugihara K, Tanigawa N. Japanese Laparoscopic Surgery Study Group. A multicenter study on oncologic outcome of laparoscopic gastrectomy for early cancer in Japan. Ann Surg. 2007. 245:68–72.
Article5. Huscher CG, Mingoli A, Sgarzini G, Sansonetti A, Di Paola M, Recher A, et al. Laparoscopic versus open subtotal gastrectomy for distal gastric cancer: five-year results of a randomized prospective trial. Ann Surg. 2005. 241:232–237.
Article6. Huscher CG, Mingoli A, Sgarzini G, Brachini G, Binda B, Di Paola M, et al. Totally laparoscopic total and subtotal gastrectomy with extended lymph node dissection for early and advanced gastric cancer: early and long-term results of a 100-patient series. Am J Surg. 2007. 194:839–844.
Article7. Tanimura S, Higashino M, Fukunaga Y, Kishida S, Ogata A, Fujiwara Y, et al. Laparoscopic gastrectomy with regional lymph node dissection for upper gastric cancer. Br J Surg. 2007. 94:204–207.
Article8. Kim SG, Lee YJ, Ha WS, Jung EJ, Ju YT, Jeong CY, et al. LATG with extracorporeal esophagojejunostomy: is this minimal invasive surgery for gastric cancer? J Laparoendosc Adv Surg Tech A. 2008. 18:572–578.
Article9. Usui S, Yoshida T, Ito K, Hiranuma S, Kudo SE, Iwai T. Laparoscopy-assisted total gastrectomy for early gastric cancer: comparison with conventional open total gastrectomy. Surg Laparosc Endosc Percutan Tech. 2005. 15:309–314.10. Mochiki E, Toyomasu Y, Ogata K, Andoh H, Ohno T, Aihara R, et al. Laparoscopically assisted total gastrectomy with lymph node dissection for upper and middle gastric cancer. Surg Endosc. 2008. 22:1997–2002.
Article11. Okabe H, Satoh S, Inoue H, Kondo M, Kawamura J, Nomura A, et al. Esophagojejunostomy through minilaparotomy after laparoscopic total gastrectomy. Gastric Cancer. 2007. 10:176–180.
Article12. Cheong O, Kim BS, Yook JH, Oh ST, Lim JT, Kim KJ, et al. Laparoscopic assisted total gastrectomy (LATG) with extracorporeal anastomosis and using circular Stapler for middle or upper early gastric carcinoma: reviews of single Surgeon's experience of 48 consecutive patients. J Korean Gastric Cancer Assoc. 2008. 8:27–34.
Article13. Uyama I, Sugioka A, Fujita J, Komori Y, Matsui H, Hasumi A. Laparoscopic total gastrectomy with distal pancreatosplenectomy and D2 lymphadenectomy for advanced gastric cancer. Gastric Cancer. 1999. 2:230–234.
Article14. Inaba K, Satoh S, Ishida Y, Taniguchi K, Isogaki J, Kanaya S, et al. Overlap method: novel intracorporeal esophagojejunostomy after laparoscopic total gastrectomy. J Am Coll Surg. 2010. 211:e25–e29.
Article15. Okabe H, Obama K, Tanaka E, Nomura A, Kawamura J, Nagayama S, et al. Intracorporeal esophagojejunal anastomosis after laparoscopic total gastrectomy for patients with gastric cancer. Surg Endosc. 2009. 23:2167–2171.
Article16. Bracale U, Marzano E, Nastro P, Barone M, Cuccurullo D, Cutini G, et al. Side-to-side esophagojejunostomy during totally laparoscopic total gastrectomy for malignant disease: a multicenter study. Surg Endosc. 2010. 24:2475–2479.
Article17. Usui S, Nagai K, Hiranuma S, Takiguchi N, Matsumoto A, Sanada K. Laparoscopy-assisted esophagoenteral anastomosis using endoscopic purse-string suture instrument "Endo-PSI (II)" and circular stapler. Gastric Cancer. 2008. 11:233–237.
Article18. Jeong O, Park YK. Intracorporeal circular stapling esophagojejunostomy using the transorally inserted anvil (OrVil) after laparoscopic total gastrectomy. Surg Endosc. 2009. 23:2624–2630.
Article19. Kunisaki C, Makino H, Oshima T, Fujii S, Kimura J, Takagawa R, et al. Application of the transorally inserted anvil (OrVil) after laparoscopy-assisted total gastrectomy. Surg Endosc. 2011. 25:1300–1305.
Article20. Kinoshita T, Oshiro T, Ito K, Shibasaki H, Okazumi S, Katoh R. Intracorporeal circular-stapled esophagojejunostomy using hand-sewn purse-string suture after laparoscopic total gastrectomy. Surg Endosc. 2010. 24:2908–2912.
Article21. Hur H, Kim JY, Cho YK, Han SU. Technical feasibility of robot-sewn anastomosis in robotic surgery for gastric cancer. J Laparoendosc Adv Surg Tech A. 2010. 20:693–697.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two-Layer Hand-Sewn Esophagojejunostomy in Totally Laparoscopic Total Gastrectomy for Gastric Cancer
- A Novel Technique of Hand-Sewn Purse-String Suturing by Double Ligation Method (DLM) for Intracorporeal Circular Esophagojejunostomy
- Intracorporeal Anastomosis in Laparoscopic Gastric Cancer Surgery
- Solo Intracorporeal Esophagojejunostomy Reconstruction Using a Laparoscopic Scope Holder in Single-Port Laparoscopic Total Gastrectomy for Early Gastric Cancer
- Left Dorsal Wall Anastomosis Compared with Parallel-Line Anastomosis for Intracorporeal Overlap Esophagojejunostomy during Laparoscopic Total Gastrectomy
