Clinical Outcome of Modified Laparoscopy-Assisted Proximal Gastrectomy Compared to Conventional Proximal Gastrectomy or Total Gastrectomy for Upper-Third Early Gastric Cancer with Special References to Postoperative Reflux Esophagitis
- Affiliations
-
- 1Department of Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. appe98@snu.ac.kr
- 2Cancer Research Institute, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Surgery, Myongji Hospital, Goyang, Korea.
- 4Department of Surgery, Gachon University Gil Medical Center, Incheon, Korea.
- 5Department of Surgery, Seoul National University Boramae Medical Center, Seoul, Korea.
- KMID: 2372205
- DOI: http://doi.org/10.5230/jgc.2015.15.3.191
Abstract
- PURPOSE
This study evaluated the functional and oncological outcomes of proximal gastrectomy (PG) in comparison with total gastrectomy (TG) for upper-third early gastric cancer (EGC).
MATERIALS AND METHODS
The medical records of upper-third EGC patients who had undergone PG (n=192) or TG (n=157) were reviewed. The PG group was further subdivided into patients who had undergone conventional open PG (cPG; n=157) or modified laparoscopy-assisted PG (mLAPG; n=35). Patients who had undergone mLAPG had a longer portion of their intra-abdominal esophagus preserved than patients who had undergone cPG. Surgical morbidity, recurrence, long-term nutritional status, and the incidence of reflux esophagitis were compared between the groups.
RESULTS
The rate of postoperative complications was significantly lower for PG than TG (16.7% vs. 31.2%), but the five-year overall survival rate was comparable between the two groups (99.3% vs. 96.3%). Postoperative levels of hemoglobin and albumin were significantly higher for patients who had undergone PG. However, the incidence of reflux esophagitis was higher for PG than for TG (37.4% vs. 3.7%; P<0.001). mLAPG was related to a lower incidence of reflux esophagitis after PG (P<0.001).
CONCLUSIONS
Compared to TG, PG showed an advantage in terms of postoperative morbidity and nutrition, and there was a comparable prognosis between the two procedures. Preserving the intra-abdominal esophagus may lower the incidence of reflux esophagitis associated with PG.
Keyword
MeSH Terms
Figure
-

Fig. 1 Differences between conventional proximal gastrectomy (PG) and modified laparoscopy-assisted PG (mLAPG). (A) In conventional PG, the vagus nerve was sacrificed, and pyloroplasty was performed in selective cases. The proximal resection line was made distal to the esophagus. (B) In mLAPG, we aimed to preserve the hepatic branch of the vagus nerve and not perform pyloroplasty. The proximal resection line was made at the gastroesophageal junction.

Fig. 2 Comparison of overall survival rates between the proximal gastrectomy (PG) and total gastrectomy (TG) groups.
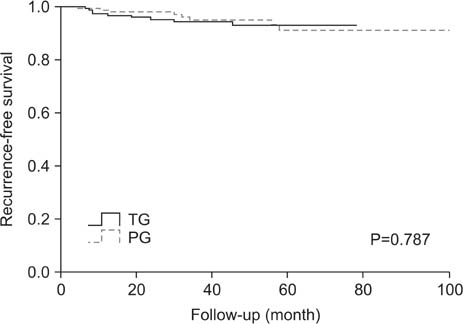
Fig. 3 Comparison of recurrence-free survival rates between the proximal gastrectomy (PG) and total gastrectomy (TG) groups.
Cited by 2 articles
-
Korean Practice Guideline for Gastric Cancer 2018: an Evidence-based, Multi-disciplinary Approach
J Gastric Cancer. 2019;19(1):1-48. doi: 10.5230/jgc.2019.19.e8.Spade-Shaped Anastomosis Following a Proximal Gastrectomy Using a Double Suture to Fix the Posterior Esophageal Wall to the Anterior Gastric Wall (SPADE Operation): Case-Control Study of Early Outcomes
Won Ho Han, Bang Wool Eom, Hong Man Yoon, Junsun Ryu, Young-Woo Kim
J Gastric Cancer. 2020;20(1):72-80. doi: 10.5230/jgc.2020.20.e5.
Reference
-
1. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011; 14:113–123.2. Harrison LE, Karpeh MS, Brennan MF. Total gastrectomy is not necessary for proximal gastric cancer. Surgery. 1998; 123:127–130.3. Katsoulis IE, Robotis JF, Kouraklis G, Yannopoulos PA. What is the difference between proximal and total gastrectomy regarding postoperative bile reflux into the oesophagus? Dig Surg. 2006; 23:325–330.4. Ahn HS, Lee HJ, Yoo MW, Jeong SH, Park DJ, Kim HH, et al. Changes in clinicopathological features and survival after gastrectomy for gastric cancer over a 20-year period. Br J Surg. 2011; 98:255–260.5. Hirai T, Matsumoto H, Iki K, Hirabayashi Y, Kawabe Y, Ikeda M, et al. Lower esophageal sphincter- and vagus-preserving proximal partial gastrectomy for early cancer of the gastric cardia. Surg Today. 2006; 36:874–878.6. Kim DJ, Lee JH, Kim W. Lower esophageal sphincter-preserving laparoscopy-assisted proximal gastrectomy in patients with early gastric cancer: a method for the prevention of reflux esophagitis. Gastric Cancer. 2013; 16:440–444.7. Armstrong D, Bennett JR, Blum AL, Dent J, De Dombal FT, Galmiche JP, et al. The endoscopic assessment of esophagitis: a progress report on observer agreement. Gastroenterology. 1996; 111:85–92.8. An JY, Youn HG, Choi MG, Noh JH, Sohn TS, Kim S. The difficult choice between total and proximal gastrectomy in proximal early gastric cancer. Am J Surg. 2008; 196:587–591.9. Katai H, Sano T, Fukagawa T, Shinohara H, Sasako M. Prospective study of proximal gastrectomy for early gastric cancer in the upper third of the stomach. Br J Surg. 2003; 90:850–853.10. Shiraishi N, Adachi Y, Kitano S, Kakisako K, Inomata M, Yasuda K. Clinical outcome of proximal versus total gastrectomy for proximal gastric cancer. World J Surg. 2002; 26:1150–1154.11. Imada T, Rino Y, Takahashi M, Suzuki M, Tanaka J, Shiozawa M, et al. Postoperative functional evaluation of pylorus-preserving gastrectomy for early gastric cancer compared with conventional distal gastrectomy. Surgery. 1998; 123:165–170.12. Park DJ, Lee HJ, Jung HC, Kim WH, Lee KU, Yang HK. Clinical outcome of pylorus-preserving gastrectomy in gastric cancer in comparison with conventional distal gastrectomy with Billroth I anastomosis. World J Surg. 2008; 32:1029–1036.13. Katai H, Sano T, Fukagawa T, Shinohara H, Sasako M. Prospective study of proximal gastrectomy for early gastric cancer in the upper third of the stomach. Br J Surg. 2003; 90:850–853.14. Uyama I, Sugioka A, Fujita J, Komori Y, Matsui H, Hasumi A. Completely laparoscopic proximal gastrectomy with jejunal interposition and lymphadenectomy. J Am Coll Surg. 2000; 191:114–119.15. Kinoshita T, Gotohda N, Kato Y, Takahashi S, Konishi M, Kinoshita T. Laparoscopic proximal gastrectomy with jejunal interposition for gastric cancer in the proximal third of the stomach: a retrospective comparison with open surgery. Surg Endosc. 2013; 27:146–153.16. Lim HJ, Jeong YJ, Yang DH. A comparative study on the outcomes of total and proximal gastrectomies performed for gastric cancer. Korean J Gastroenterol. 2002; 40:364–370.17. Pierie JP, de Graaf PW, Poen H, van der Tweel I, Obertop H. Incidence and management of benign anastomotic stricture after cervical oesophagogastrostomy. Br J Surg. 1993; 80:471–474.18. Shemesh E, Czerniak A. Comparison between Savary-Gilliard and balloon dilatation of benign esophageal strictures. World J Surg. 1990; 14:518–521. discussion 521-52219. Brandimarte G, Tursi A. Endoscopic treatment of benign anastomotic esophageal stenosis with electrocautery. Endoscopy. 2002; 34:399–401.20. Hordijk ML, Siersema PD, Tilanus HW, Kuipers EJ. Electrocautery therapy for refractory anastomotic strictures of the esophagus. Gastrointest Endosc. 2006; 63:157–163.21. Bae JM, Park JW, Kim JP. Nutritional assessment and intestinal absorption studies on total gastrectomized gastric cancer patients. J Korean Surg Soc. 1996; 50:475–487.22. Cho SJ, Jegal YJ. Nutritional status, and mucosal morphology of jejunum after total gastrectomy for carcinoma of the stomach. J Korean Surg Soc. 1990; 39:726–734.23. Kim JW, Yoon H, Kong SH, Kim JS, Paeng JC, Lee HJ, et al. Analysis of esophageal reflux after proximal gastrectomy measured by wireless ambulatory 24-hr esophageal pH monitoring and TC-99m diisopropyliminodiacetic acid (DISIDA) scan. J Surg Oncol. 2010; 101:626–633.24. Sakuramoto S, Yamashita K, Kikuchi S, Futawatari N, Katada N, Moriya H, et al. Clinical experience of laparoscopy-assisted proximal gastrectomy with Toupet-like partial fundoplication in early gastric cancer for preventing reflux esophagitis. J Am Coll Surg. 2009; 209:344–351.25. Ichikawa D, Komatsu S, Okamoto K, Shiozaki A, Fujiwara H, Otsuji E. Evaluation of symptoms related to reflux esophagitis in patients with esophagogastrostomy after proximal gastrectomy. Langenbecks Arch Surg. 2013; 398:697–701.26. Nakamura M, Nakamori M, Ojima T, Katsuda M, Iida T, Hayata K, et al. Reconstruction after proximal gastrectomy for early gastric cancer in the upper third of the stomach: an analysis of our 13-year experience. Surgery. 2014; 156:57–63.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single-Port Laparoscopic Proximal Gastrectomy with Double Tract Reconstruction for Early Gastric Cancer: Report of a Case
- Laparoscopic Proximal Gastrectomy as a Surgical Treatment for Upper Third Early Gastric Cancer
- The Risk Factors of Reflux Complication after Gastrectomy for Proximal Gastric Cancer
- Long-term Results of Proximal and Total Gastrectomy for Adenocarcinoma of the Upper Third of the Stomach
- Non-Randomized Confirmatory Trial of Laparoscopy-Assisted Total Gastrectomy and Proximal Gastrectomy with Nodal Dissection for Clinical Stage I Gastric Cancer: Japan Clinical Oncology Group Study JCOG1401
