Treatment of Avulsion Fracture of Proximal Rectus Femoris with Suture Anchor
- Affiliations
-
- 1Department of Orthopaedic Surgery, Dong-Eui Medical Center, Busan, Korea. hangulum@hanmail.net
- 2Department of Orthopaedic Surgery, Barun Hospital, Jinju, Korea.
- KMID: 2361674
- DOI: http://doi.org/10.5763/kjsm.2016.34.1.83
Abstract
- Avulsion injuries of the anterior inferior iliac spine, which is the origin of the rectus femoris muscle, are sometimes reported in children and adolescents, but acute avulsion injuries with complete rupture of the rectus femoris are very rare in adults. We treated a case of avulsion fracture of the anterior inferior iliac spine with suture anchors in an adult and achieved a favorable outcome. Thus, we report the case with a review of literature.
Figure
-

Fig. 1. Simple AP radiograph shows an avulsed bone fragment displaced inferiorly from the right anterior inferior iliac spine (arrow).

Fig. 2. T2-weighted coronal magnetic resonance image shows complete avulsion of the direct head of the right rectus femoris muscle (arrow) and severe edematous change (arrow heads).
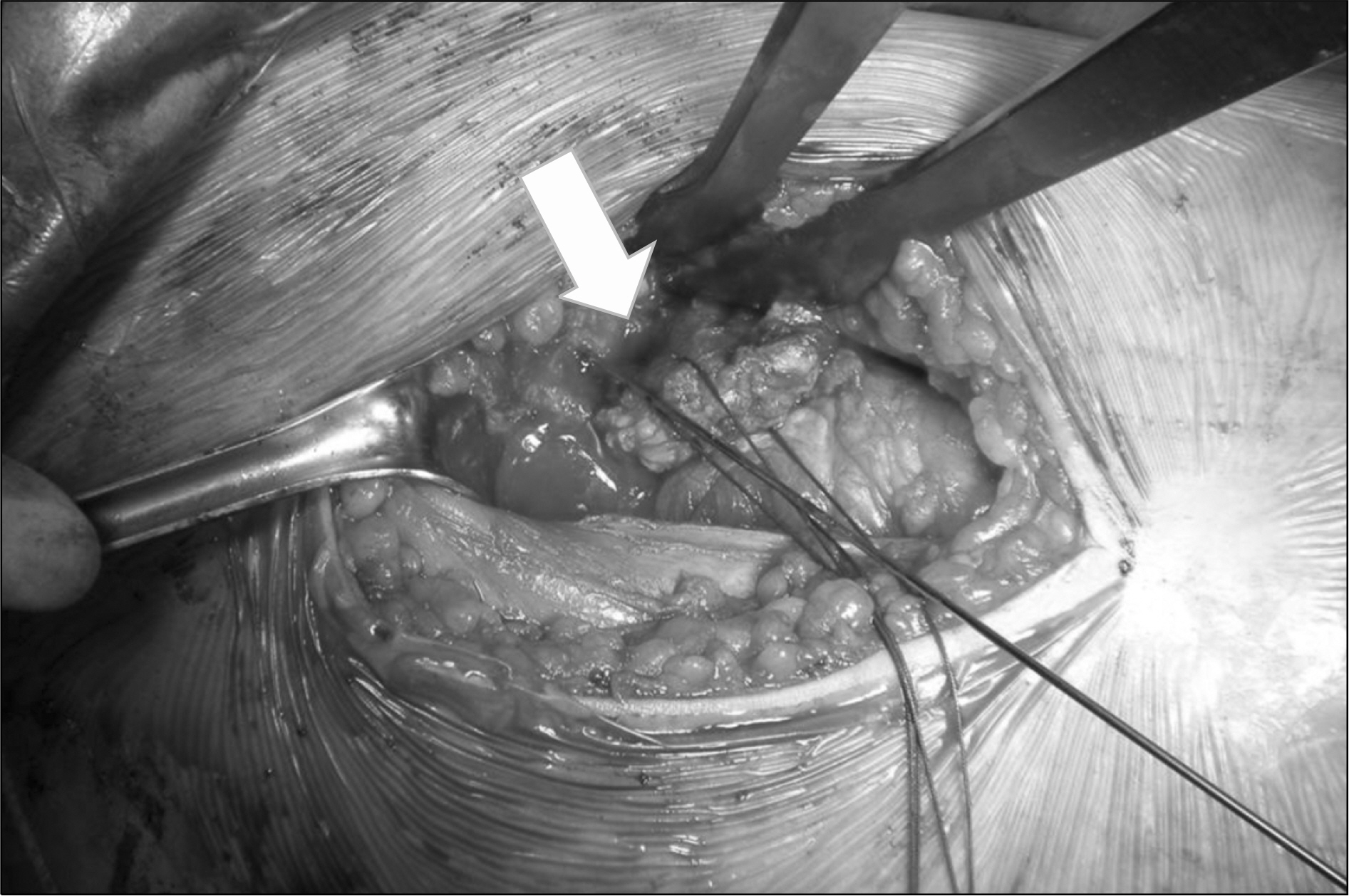
Fig. 3. During the operation, the detached bone fragment from the anterior inferior iliac spine is seen between the tensor fasciae latae and the sartorius, with the rectus femoris distally displaced by 2.5 cm (arrow).

Fig. 4. The displaced fragment was reduced with two suture anchors through the modified Kessler technique (arrow).

Fig. 5. Simple AP radiograph checked 4 months after the operation shows a healed avulsed bony fragment without inferior displacement (arrow).
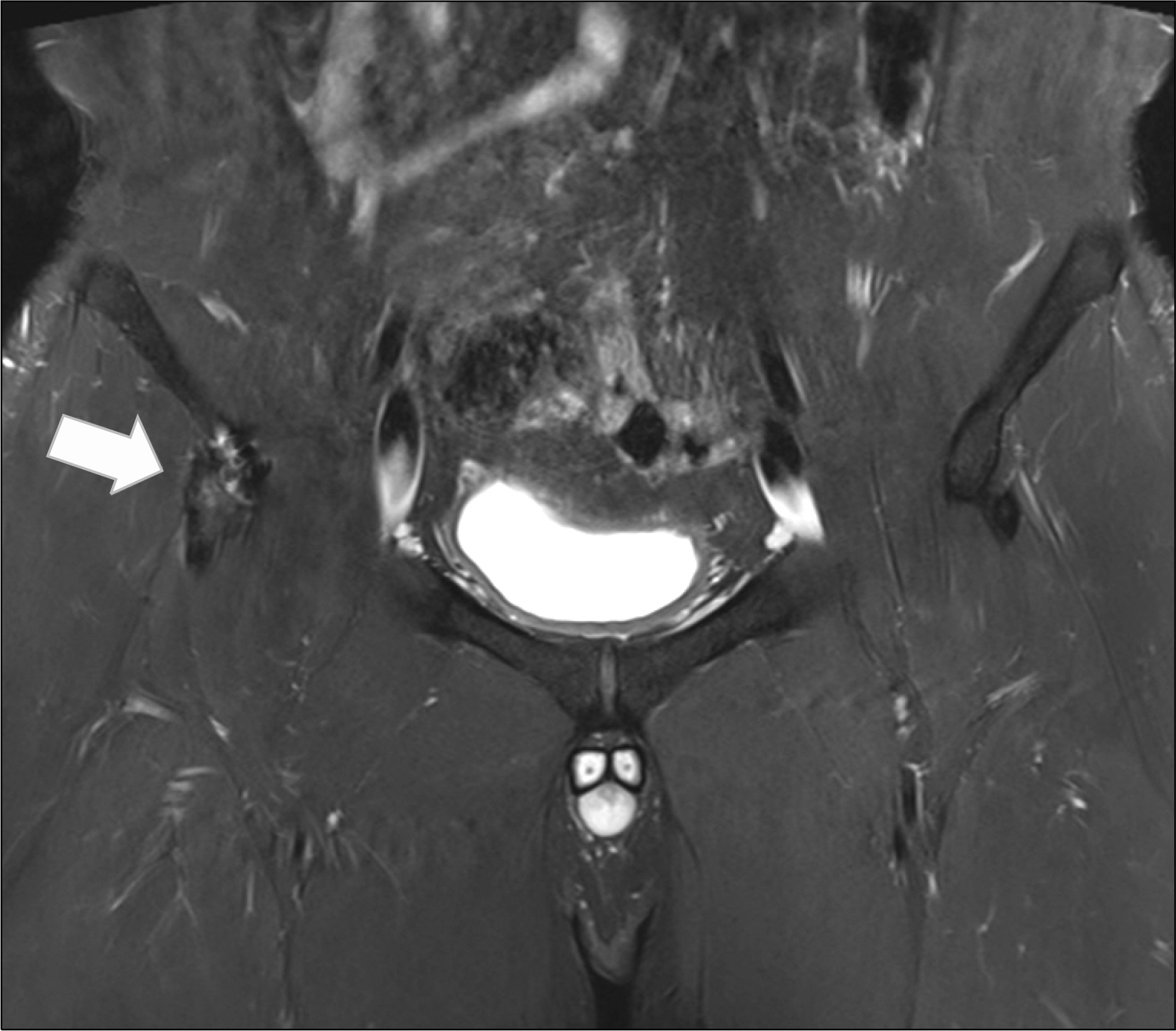
Fig. 6. T2-weighted coronal magnetic resonance image checked 4 months after the operation shows anatomical restoration of the direct head of the right rectus femoris muscle (arrow).
Reference
-
1.Zarins B., Ciullo JV. Acute muscle and tendon injuries in athletes. Clin Sports Med. 1983. 2:167–82.
Article2.Rajasekhar C., Kumar KS., Bhamra MS. Avulsion fractures of the anterior inferior iliac spine: the case for surgical intervention. Int Orthop. 2001. 24:364–5.
Article3.Gomez JE. Bilateral anterior inferior iliac spine avulsion fractures. Med Sci Sports Exerc. 1996. 28:161–4.
Article4.Mader TJ. Avulsion of the rectus femoris tendon: an unusual type of pelvic fracture. Pediatr Emerg Care. 1990. 6:198–9.5.Renstrom PA. Tendon and muscle injuries in the groin area. Clin Sports Med. 1992. 11:815–31.
Article6.Cross TM., Gibbs N., Houang MT., Cameron M. Acute quadriceps muscle strains: magnetic resonance imaging features and prognosis. Am J Sports Med. 2004. 32:710–9.7.Jeon SJ., Jeon HS., Moon CS., Noh HK., Ha SJ. Complete rupture of the origins of rectus femoris occurred during relay race: a case report. J Korean Orthop Soc Sports Med. 2008. 7:151–5.8.Milankov MZ., Harhaji V., Gojkovic Z., Drapsin M. Heterotopic ossification following surgical treatment of avulsion fracture of the anterior inferior iliac spine. Med Pregl. 2011. 64:593–6.
Article9.Knobloch K., Kramer R., Sommer K., Gansslen A., Vogt PM. Avulsion injuries of the anterior inferior iliac spine among soccer players: a differential diagnosis to neoplasm decades following the trauma. Sportverletz Sportschaden. 2007. 21:152–6.10.Sundar M., Carty H. Avulsion fractures of the pelvis in children: a report of 32 fractures and their outcome. Skeletal Radiol. 1994. 23:85–90.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Osteolysis-Related Bioabsorbable Suture Anchor Fixation in a Medial Collateral Ligament Avulsion Fracture during Total Knee Arthroplasty
- Treatment of Acetabular Avulsion Fracture with Labral Tear Using Suture Anchor: A Case Report
- Mini-Plate and Screw Fixation Technique for Comminuted Flexor Digitorum Profundus Avulsion Fracture
- Arthroscopic Bio-Absorbable Suture Anchor Fixation of Tibial Eminence Avulsion Fracture in Children
- Suture Bridge Fixation Technique for Posterior Cruciate Ligament Avulsion Fracture
