Sonographic Findings of Common Musculoskeletal Diseases in Patients with Diabetes Mellitus
- Affiliations
-
- 1Department of Medicine, Graduate School, Kyung Hee University, Seoul 02447, Korea.
- 2Department of Radiology, Kyung Hee University Hospital, Seoul 02447, Korea. francesca@hanmail.net
- 3Department of Radiology, Kyung Hee University Hospital at Gangdong, Seoul 05278, Korea.
- KMID: 2360210
- DOI: http://doi.org/10.3348/kjr.2016.17.2.245
Abstract
- Diabetes mellitus (DM) can accompany many musculoskeletal (MSK) diseases. It is difficult to distinguish the DM-related MSK diseases based on clinical symptoms alone. Sonography is frequently used as a first imaging study for these MSK symptoms and is helpful to differentiate the various DM-related MSK diseases. This pictorial essay focuses on sonographic findings of various MSK diseases that can occur in diabetic patients.
Keyword
MeSH Terms
-
Adult
Cellulitis/ultrasonography
Diabetes Mellitus, Type 2/*complications
Diabetic Neuropathies/ultrasonography
Female
Humans
Male
Musculoskeletal Diseases/complications/*diagnosis/ultrasonography
Pyomyositis/microbiology/ultrasonography
Tenosynovitis/microbiology/ultrasonography
Vascular Diseases/ultrasonography
Figure
-

Fig. 1 Cellulitis with abscess formation of right foot in 49-year-old patient with painful swelling and fever. A. Longitudinal sonography scan shows diffuse thickening of subcutaneous tissues with large subcutaneous fluid collection (arrows) filled with echogenic material (asterisk). B. Transverse color Doppler sonography scan shows increased vascularity surrounding multiloculated, hypoechoic fluid collection. Streptococcus viridans was cultured from fluid obtained with sonography-guided aspiration. C. Sagittal enhanced T1-weighted fat-suppressed image shows subcutaneous fluid collection with rim-like enhancement. Drain tube is inserted at fluid collection (arrow). Surrounding edema without involvement of deep soft tissue or bony structure is noted.
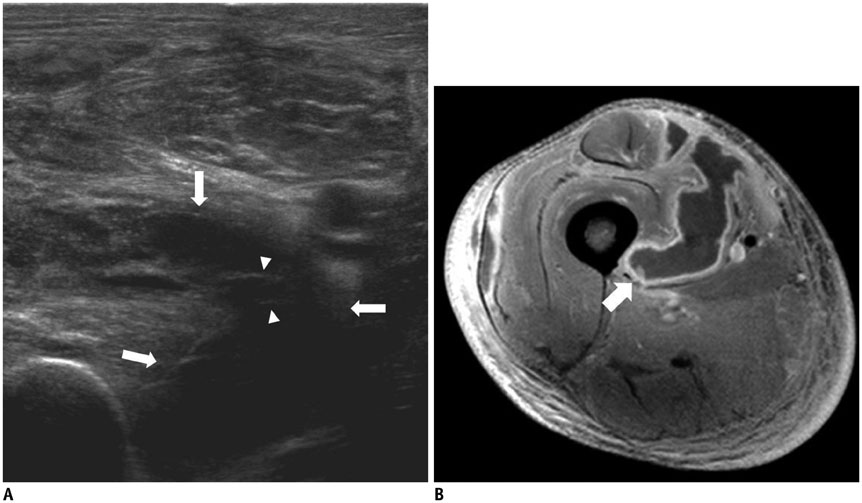
Fig. 2 Infectious pyomyositis with intramuscular abscess due to Staphylococcus aureus in 36-year-old patient with right thigh pain and fever. A. Transverse sonography scan of medial thigh shows fluid collection (arrows) with echogenic septa (arrowheads) within vastus medialis muscle. Diffuse edema of adjacent muscles and subcutaneous layer are also noted. B. Axial enhanced T1-weighted fat-suppressed image shows few fluid collections with rim-like enhancement within vastus medialis (arrow), vastus lateralis, and rectus femoris.
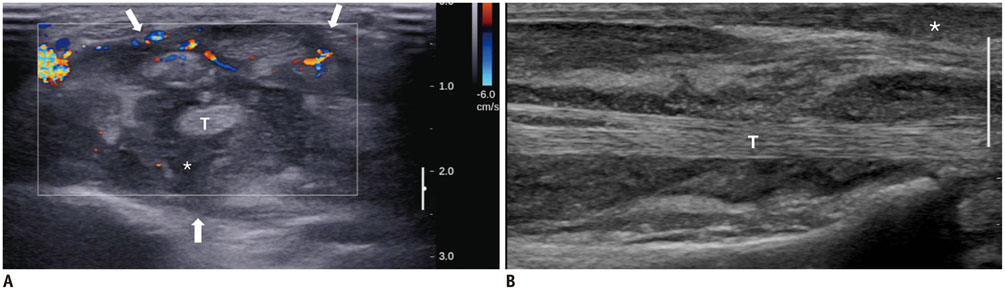
Fig. 3 Infectious pyomyositis, tenosynovitis, and cellulitis with abscess due to tuberculosis in 61-year-old patient with right forearm pain and fever. A. Transverse color Doppler sonography scan at distal radioulnar joint level shows distended flexor tendon sheath (arrows) filled with echogenic debris (asterisk) and hypervascularity. Tendons are mildly thickened. B. Longitudinal sonography scan reveals subcutaneous extension of echogenic debris (asterisk), suggesting ruptured tendon sheath. T = tendon
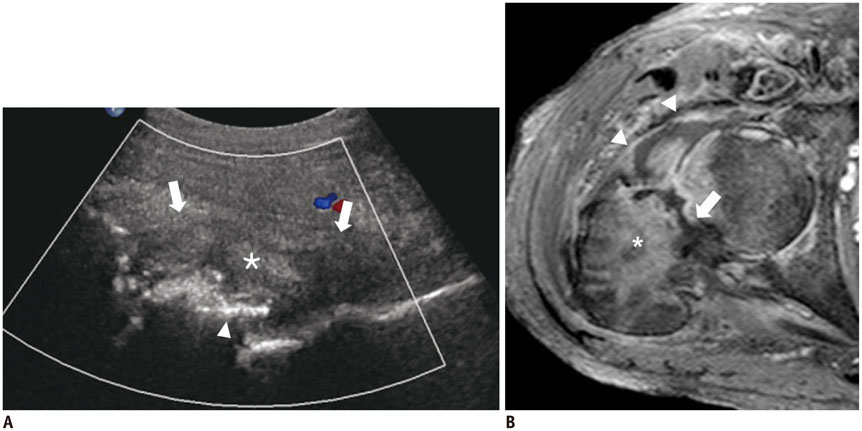
Fig. 4 Septic arthritis of right hip in 57-year-old patient with hip pain and fever. A. Longitudinal sonography scan of anterior aspect of right hip joint shows joint distension (arrows), bone destruction (arrowhead), and fluid with echogenic debris (asterisk) with adjacent soft tissue edema. B. Axial enhanced T1-weighted fat-suppressed image shows septic arthritis of right hip and osteomyelitis (asterisk) with pathologic fracture of femur (arrow). Joint fluid and irregular synovial enhancement (arrowheads) are seen.

Fig. 5 Medial arteriosclerosis showing stiff Doppler flow pattern in lower extremity in 60-year-old patient. A. Longitudinal sonography scan of superficial femoral artery shows continuous echogenic lines (arrows) in vessel wall without luminal narrowing. Doppler flow pattern shows decreased 2nd reversal flow in early diastole and loss of 3rd wave. These findings are suggestive of decreased resistance of distal arteries and arterial stiffness. B. Plain radiography of left knee shows continuous circumferential fine calcification along superficial femoral artery and popliteal tributaries (arrows).

Fig. 6 Neuropathic osteoarthropathy with combined infection (Pseudomonas aeruginosa) of left knee in 61-year-old patient with knee swelling. A. Transverse sonography scan of suprapatellar bursa shows large amount of joint effusion filled with echogenic material (asterisk) and diffuse thickening of subcutaneous tissues. B. Longitudinal sonography scan of medial aspect of left knee shows cortical destruction of tibia (arrows) and joint effusion with echogenic materials. C. Plain radiography of left knee shows severe bone destruction with discrete margin, fragmentations, joint subluxation, and soft tissue edema. Serial radiographs (not shown) demonstrate rapid progression of bone destruction.
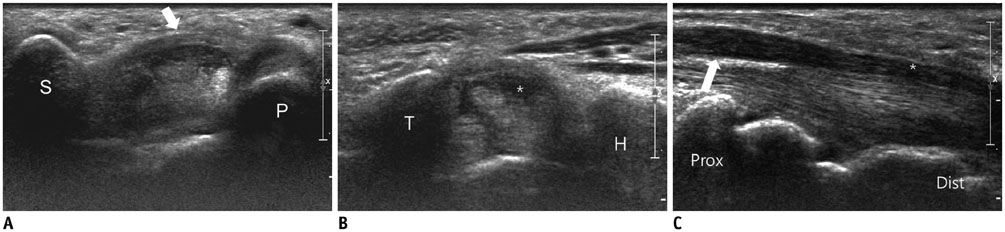
Fig. 7 Carpal tunnel syndrome of left wrist in 58-year-old patient with complaint of tingling sensation of both hands. A. Transverse sonography of left wrist scan shows palmar bowing of flexor retinaculum at proximal carpal tunnel level delimited by scaphoid (S) and pisiform (P). Diffuse thickening of flexor retinaculum is noted (arrow). B. Transverse sonography scan shows median nerve flattening (asterisk) at distal carpal tunnel level delimited by hamate (H) and trapezium (T). C. Longitudinal sonography scan shows median nerve flattening (asterisk) at distal (dist) carpal tunnel level and median nerve swelling (arrow) at distal radius level (prox). Surgical release of carpal tunnel was performed because of non-responsiveness to conservative management.
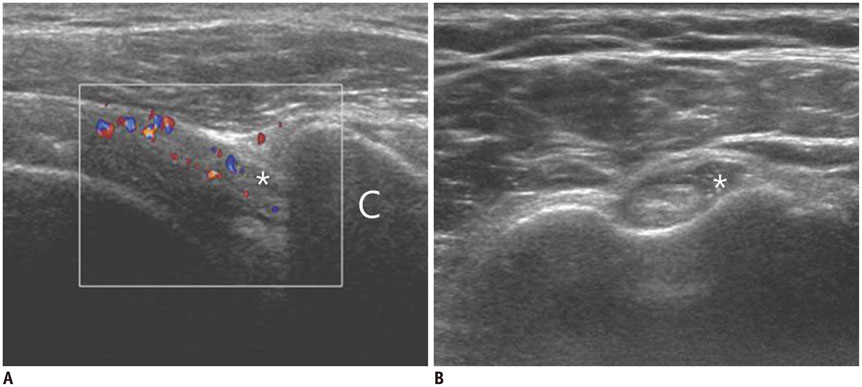
Fig. 8 Adhesive capsulitis of right shoulder in 49-year-old patient with bilateral shoulder pain. A. Transverse color Doppler sonography scan shows thickening of cuff interval structures with increased vascularity (asterisk). Dynamic sonography scan of right shoulder shows marked limitation of sliding movement of supraspinatus tendon beneath acromion during lateral passive elevation of arm (not visualized in this figure). B. Transverse sonography scan shows distension of biceps long head tendon sheath (asterisk) with joint fluid collection. C = coracoid process
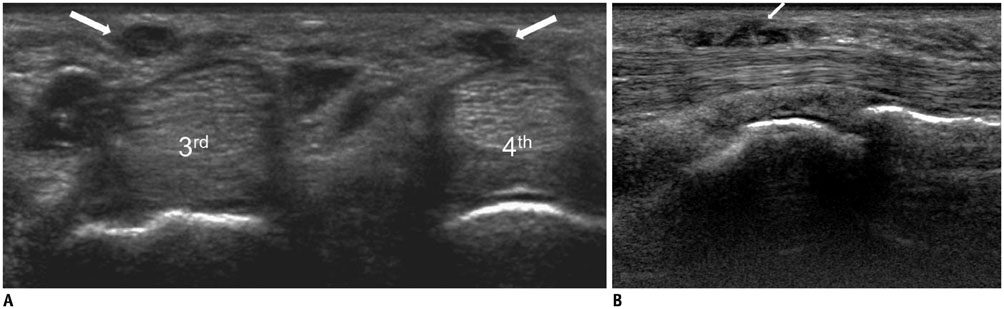
Fig. 9 Dupuytren's contracture of right hand in 48-year-old patient complaint of contracture of right 4th finger and palpable nodules on palm. A. Transverse sonography scans shows hypoechoic nodular lesions (arrows) in subcutaneous fat layer of right palm at 3rd and 4th metacarpal head level, suggesting nodular thickening of palmar fascia. B. On longitudinal sonography scan, subcutaneous cord (arrow) at distal crease level is contiguous with thickened tendon sheath of 4th flexor digitorum tendon. 3rd = 3rd metacarpal head, 4th = 4th metacarpal head

Fig. 10 Trigger finger affecting right 2nd–4th fingers in 38-year-old patient with difficulty in extension of right 2nd–4th fingers. A. Transverse sonography scan shows hypoechoic nodular thickening of first annular pulleys (arrows) at metacarpophalangeal joint level. B. Longitudinal sonography scan shows blurred margin of 2nd flexor digitorum tendon (arrow). 2nd = 2nd flexor digitorum tendon, 3rd = 3rd flexor digitorum tendon, 4th = 4th flexor digitorum tendon, MC = 2nd metacarpal bone, P = 2nd proximal phalanx

Fig. 11 Diabetic muscle infarction affecting right thigh in 55-year-old patient with leg pain. A, B. Transverse (A) and longitudinal (B) sonography scans show heterogeneous echogenicity of right vastus lateralis muscle. On longitudinal scan (B), hypoechoic portion with preservation of echogenic fibrillar pattern of muscle fibers (arrow) is noted. Significant fluid collection is absent. C. Axial T2-weighted MR image shows diffuse edema of right vastus lateralis muscle. Note focal T2 low signal intensity lesion (arrow). D. On axial enhanced T1-weighted fat-suppressed MR image, focal T2 low signal lesion corresponds to lesion with decreased enhancement and surrounding enhancement (arrow).
Reference
-
1. Joshi N, Caputo GM, Weitekamp MR, Karchmer AW. Infections in patients with diabetes mellitus. N Engl J Med. 1999; 341:1906–1912.2. Casqueiro J, Casqueiro J, Alves C. Infections in patients with diabetes mellitus: a review of pathogenesis. Indian J Endocrinol Metab. 2012; 16:Suppl 1. S27–S36.3. Chau CL, Griffith JF. Musculoskeletal infections: ultrasound appearances. Clin Radiol. 2005; 60:149–159.4. Turecki MB, Taljanovic MS, Stubbs AY, Graham AR, Holden DA, Hunter TB, et al. Imaging of musculoskeletal soft tissue infections. Skeletal Radiol. 2010; 39:957–971.5. Patel SR, Olenginski TP, Perruquet JL, Harrington TM. Pyomyositis: clinical features and predisposing conditions. J Rheumatol. 1997; 24:1734–1738.6. Bosshardt TL, Henderson VJ, Organ CH Jr. Necrotizing soft-tissue infections. Arch Surg. 1996; 131:846–852. discussion 852-8547. Wongworawat MD, Holtom P, Learch TJ, Fedenko A, Stevanovic MV. A prolonged case of Mycobacterium marinum flexor tenosynovitis: radiographic and histological correlation, and review of the literature. Skeletal Radiol. 2003; 32:542–545.8. Bellapianta JM, Ljungquist K, Tobin E, Uhl R. Necrotizing fasciitis. J Am Acad Orthop Surg. 2009; 17:174–182.9. Bureau NJ, Ali SS, Chhem RK, Cardinal E. Ultrasound of musculoskeletal infections. Semin Musculoskelet Radiol. 1998; 2:299–306.10. Andras A, Ferket B. Screening for peripheral arterial disease. Cochrane Database Syst Rev. 2014; 4:CD010835.11. Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA. 2002; 287:2570–2581.12. Gibbons GW, Shaw PM. Diabetic vascular disease: characteristics of vascular disease unique to the diabetic patient. Semin Vasc Surg. 2012; 25:89–92.13. Pectasides M, Kalva SP. Diabetes revealed: multisystem danger. AJR Am J Roentgenol. 2011; 196:274–286.14. Schäberle W. Ultrasonography in Vascular Diagnosis: A Therapy-Oriented Textbook and Atlas. Berlin: Springer-Verlag;2011. p. 258.15. Al-Aly Z. Medial vascular calcification in diabetes mellitus and chronic kidney disease: the role of inflammation. Cardiovasc Hematol Disord Drug Targets. 2007; 7:1–6.16. David Smith C, Gavin Bilmen J, Iqbal S, Robey S, Pereira M. Medial artery calcification as an indicator of diabetic peripheral vascular disease. Foot Ankle Int. 2008; 29:185–190.17. Liu KH, Chu WC, Kong AP, Choi Ko GT, Ma RC, Chan JW, et al. US assessment of medial arterial calcification: a sensitive marker of diabetes-related microvascular and macrovascular complications. Radiology. 2012; 265:294–302.18. Puttemans T, Nemery C. Diabetes: the use of color Doppler sonography for the assessment of vascular complications. Eur J Ultrasound. 1998; 7:15–22.19. Thakkar RS, Del Grande F, Thawait GK, Andreisek G, Carrino JA, Chhabra A. Spectrum of high-resolution MRI findings in diabetic neuropathy. AJR Am J Roentgenol. 2012; 199:407–412.20. Tan PL, Teh J. MRI of the diabetic foot: differentiation of infection from neuropathic change. Br J Radiol. 2007; 80:939–948.21. Jones EA, Manaster BJ, May DA, Disler DG. Neuropathic osteoarthropathy: diagnostic dilemmas and differential diagnosis. Radiographics. 2000; 20 Spec No:S279–S293.22. Baker JC, Demertzis JL, Rhodes NG, Wessell DE, Rubin DA. Diabetic musculoskeletal complications and their imaging mimics. Radiographics. 2012; 32:1959–1974.23. Bianchi S, Baert AL, Abdelwahab IF, Derchi LE, Martinoli C, Rizzatto G, et al. Ultrasound of the musculoskeletal system. Heidelberg: Springer;2007. p. 862.24. Schweitzer ME, Daffner RH, Weissman BN, Bennett DL, Blebea JS, Jacobson JA, et al. ACR Appropriateness Criteria on suspected osteomyelitis in patients with diabetes mellitus. J Am Coll Radiol. 2008; 5:881–886.25. Fitzgibbons PG, Weiss AP. Hand manifestations of diabetes mellitus. J Hand Surg Am. 2008; 33:771–775.26. Resnick D, Kransdorf M. Bone and Joint Imaging. 3rd ed. Philadelphia: Elsevier Saunders;2005. p. 625–629.27. Thomsen NO, Cederlund R, Rosén I, Björk J, Dahlin LB. Clinical outcomes of surgical release among diabetic patients with carpal tunnel syndrome: prospective follow-up with matched controls. J Hand Surg Am. 2009; 34:1177–1187.28. Mallouhi A, Pülzl P, Trieb T, Piza H, Bodner G. Predictors of carpal tunnel syndrome: accuracy of gray-scale and color Doppler sonography. AJR Am J Roentgenol. 2006; 186:1240–1245.29. Huang YP, Fann CY, Chiu YH, Yen MF, Chen LS, Chen HH, et al. Association of diabetes mellitus with the risk of developing adhesive capsulitis of the shoulder: a longitudinal population-based followup study. Arthritis Care Res (Hoboken). 2013; 65:1197–1202.30. Jacobson JA. Musculoskeletal ultrasound: focused impact on MRI. AJR Am J Roentgenol. 2009; 193:619–627.31. Papatheodorou A, Ellinas P, Takis F, Tsanis A, Maris I, Batakis N. US of the shoulder: rotator cuff and non-rotator cuff disorders. Radiographics. 2006; 26:e23.32. Murphey MD, Ruble CM, Tyszko SM, Zbojniewicz AM, Potter BK, Miettinen M. From the archives of the AFIP: musculoskeletal fibromatoses: radiologic-pathologic correlation. Radiographics. 2009; 29:2143–2173.33. Khashan M, Smitham PJ, Khan WS, Goddard NJ. Dupuytren’s disease: review of the current literature. Open Orthop J. 2011; 5:Suppl 2. 283–288.34. Créteur V, Madani A, Gosset N. [Ultrasound imaging of Dupuytren’s contracture]. J Radiol. 2010; 91:687–691.35. Ryzewicz M, Wolf JM. Trigger digits: principles, management, and complications. J Hand Surg Am. 2006; 31:135–146.36. Kim HR, Lee SH. Ultrasonographic assessment of clinically diagnosed trigger fingers. Rheumatol Int. 2010; 30:1455–1458.37. Delaney-Sathy LO, Fessell DP, Jacobson JA, Hayes CW. Sonography of diabetic muscle infarction with MR imaging, CT, and pathologic correlation. AJR Am J Roentgenol. 2000; 174:165–169.38. Trujillo-Santos AJ. Diabetic muscle infarction: an underdiagnosed complication of long-standing diabetes. Diabetes Care. 2003; 26:211–215.39. Parmar MS. Diabetic muscle infarction. BMJ. 2009; 338:b2271.
