Cerebral Angiographic Findings of Cosmetic Facial Filler-related Ophthalmic and Retinal Artery Occlusion
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. sejoon1@snu.ac.kr
- 2Department of Ophthalmology, Hallym University College of Medicine, Kangdong Sacred Heart Hospital, Seoul, Korea.
- 3Department of Radiology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2359971
- DOI: http://doi.org/10.3346/jkms.2015.30.12.1847
Abstract
- Cosmetic facial filler-related ophthalmic artery occlusion is rare but is a devastating complication, while the exact pathophysiology is still elusive. Cerebral angiography provides more detailed information on blood flow of ophthalmic artery as well as surrounding orbital area which cannot be covered by fundus fluorescein angiography. This study aimed to evaluate cerebral angiographic features of cosmetic facial filler-related ophthalmic artery occlusion patients. We retrospectively reviewed cerebral angiography of 7 patients (4 hyaluronic acid [HA] and 3 autologous fat-injected cases) showing ophthalmic artery and its branches occlusion after cosmetic facial filler injections, and underwent intra-arterial thrombolysis. On selective ophthalmic artery angiograms, all fat-injected patients showed a large filling defect on the proximal ophthalmic artery, whereas the HA-injected patients showed occlusion of the distal branches of the ophthalmic artery. Three HA-injected patients revealed diminished distal runoff of the internal maxillary and facial arteries, which clinically corresponded with skin necrosis. However, all fat-injected patients and one HA-injected patient who were immediately treated with subcutaneous hyaluronidase injection showed preserved distal runoff of the internal maxillary and facial arteries and mild skin problems. The size difference between injected materials seems to be associated with different angiographic findings. Autologous fat is more prone to obstruct proximal part of ophthalmic artery, whereas HA obstructs distal branches. In addition, hydrophilic and volume-expansion property of HA might exacerbate blood flow on injected area, which is also related to skin necrosis. Intra-arterial thrombolysis has a limited role in reconstituting blood flow or regaining vision in cosmetic facial filler-associated ophthalmic artery occlusions.
Keyword
MeSH Terms
-
Adipose Tissue/transplantation
Adult
Aged
Arterial Occlusive Diseases/*etiology/*radiography/therapy
Cerebral Angiography
Cosmetic Techniques/adverse effects
Dermal Fillers/administration & dosage/*adverse effects
Face
Female
Humans
Hyaluronic Acid/administration & dosage/adverse effects
Hyaluronoglucosaminidase/administration & dosage
Injections, Subcutaneous
Ophthalmic Artery/*radiography
Retinal Artery Occlusion/*etiology/*radiography/therapy
Retrospective Studies
Transplantation, Autologous/adverse effects
Young Adult
Dermal Fillers
Hyaluronic Acid
Hyaluronoglucosaminidase
Figure
-
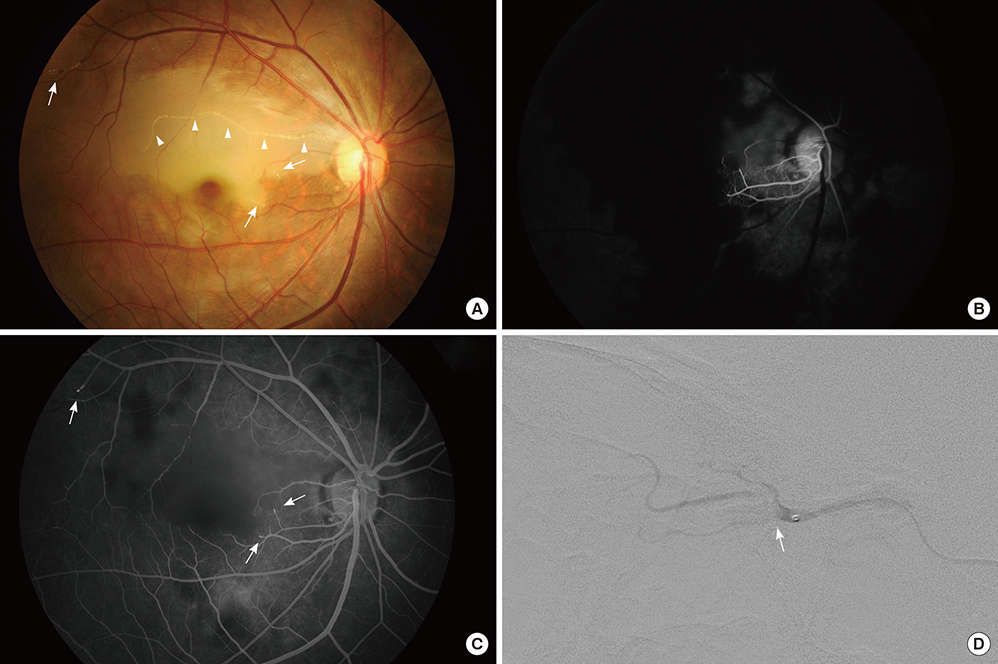
Fig. 1 Angiographic findings of an autologous fat-injected patient. A 40-yr-old woman after autologous fat injection in the glabella. (A) The fundus photograph shows an obstructed retinal artery with white infiltrations (arrow heads) and retinal edema at the corresponding area. Some whitish infiltration is observed at the end of arterioles (arrows). (B) Fluorescein angiography reveals markedly delayed retinal and choroidal perfusion. (C) There is abrupt cut off of some of the arteriolar ends (arrows), and demonstrates focal hyperfluorescence in the late phase, which suggests direct embolic obstruction of the arteriole. (D) The selective ophthalmic artery angiogram shows a large filling defect (arrow) in the proximal ophthalmic artery.
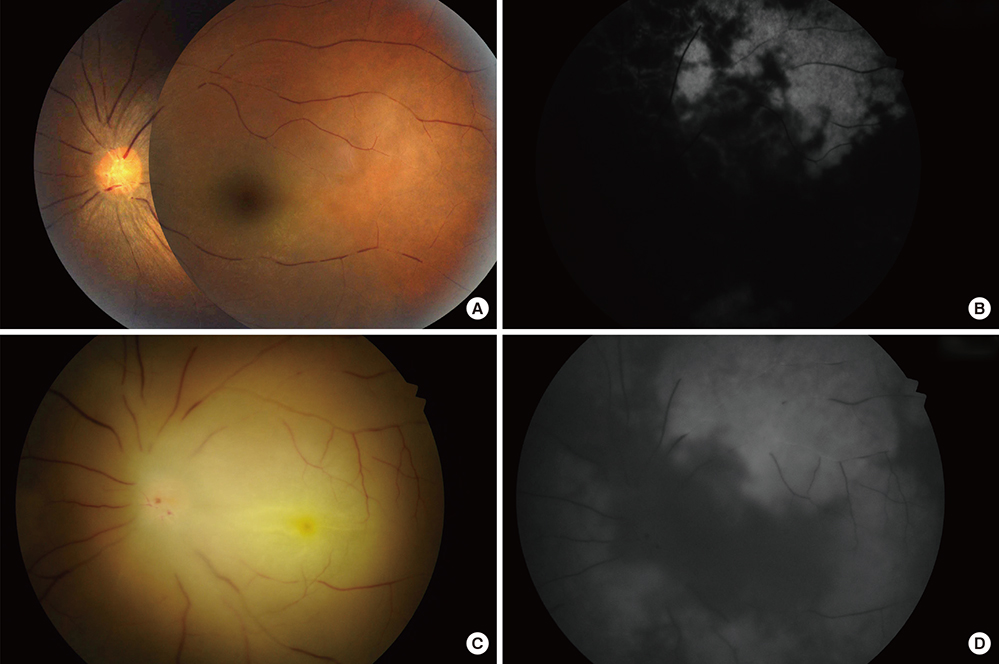
Fig. 2 Angiographic findings of a hyaluronic acid-injected patient. A 39-yr-old woman after hyaluronic acid injection in the glabella and nasal dorsum. (A) Fundus photograph reveals segmented and attenuated retinal vessels. (B) Fundus fluorescein angiography shows markedly compromised retinal and choroidal perfusion. (C) Fundus photograph taken at the day after intra-arterial thrombolysis. The retinal vessels were still segmented and the margin was blurred due to retinal edema secondary to ischemic injury. (D) The choroidal perfusion was improved after intra-arterial thrombolysis, while retinal perfusion remained compromised.
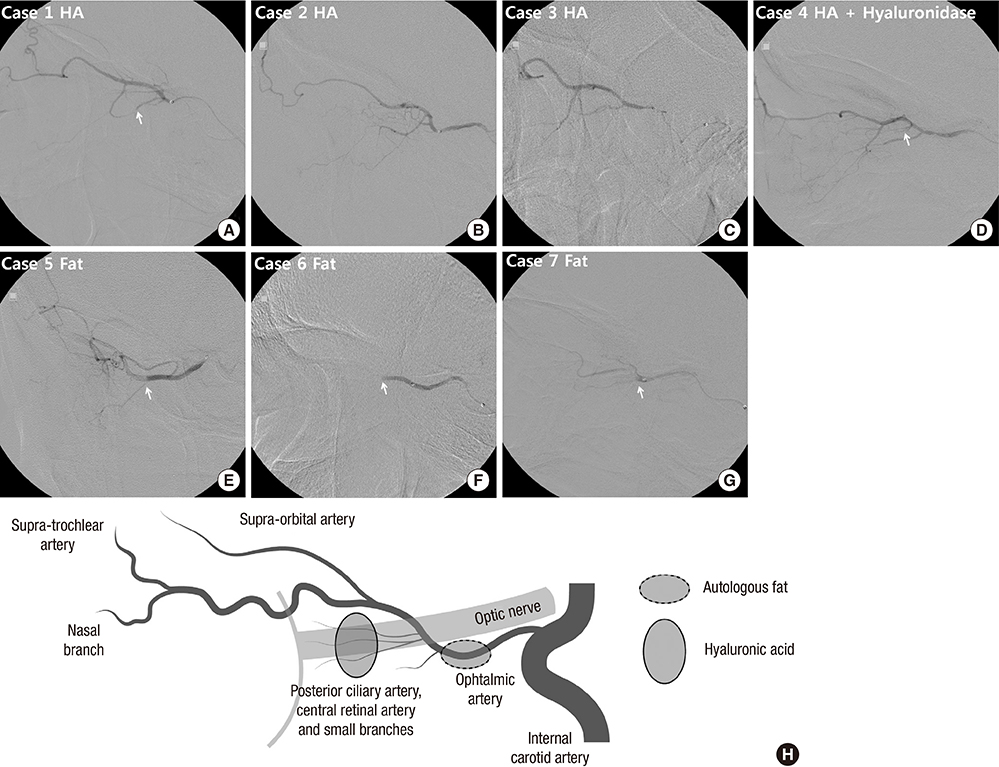
Fig. 3 Selective ophthalmic artery angiogram. (A-D) In hyaluronic acid-injected patients, no mechanical obstruction is visible in the supratrochlear or supraorbital branch, while blood flow to the retina and the choroid is compromised. (A and D) Obstruction was visible in two patients at small branches of the second segment of ophthalmic artery including the posterior ciliary branch (arrow). (B and C) However, it could not be clearly delineated in the other two patients. (E-G) In autologous fat-injected patients, a large filling defect is visible in the proximal part of ophthalmic artery (arrow). Blood flow is compromised thereafter. (H) Schematic drawings of the vascular anatomy in selective ophthalmic artery angiogram. The lighter lines indicate the optic nerve and the posterior wall of the eye ball. Presumed obstruction level is shown as dashed circle (autologous fat) or lined circle (hyaluronic acid). Case numbers are identical to those in Table 1.

Fig. 4 Selective external carotid artery angiogram. (A-C) In hyaluronic acid-injected patients, the angiographic runoff is diminished in the distal branches of internal maxillary and/or facial arteries and contrast staining is decreased in the periorbital area (dashed circle). (C) Faint distal runoff of internal maxillary artery (arrows) is observed but periorbital contrast staining is diminished (dashed circle). (D-G) In hyaluronic acid-injected patient, who were also treated with subcutaneous hyaluronidase injection (D), and in autologous fat-injected patients (E-G), the distal angiographic runoff in the distal branches of internal maxillary and/or facial arteries (arrows) and contrast staining (arrow heads) are relatively preserved (dashed circle). Case numbers are identical to those in Table 1.
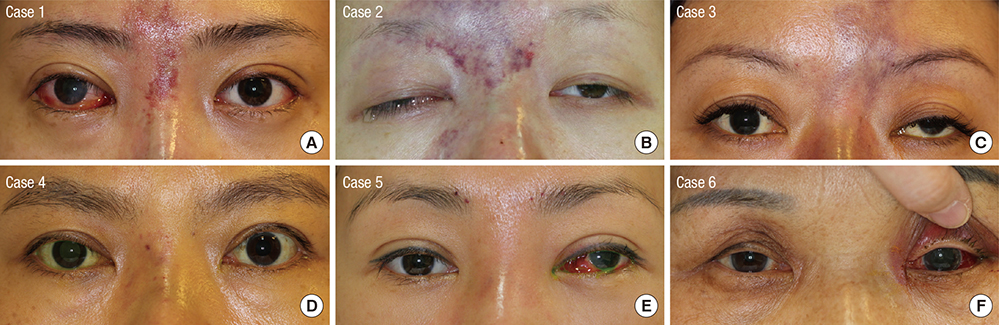
Fig. 5 Skin changes after cosmetic facial filler injections on the glabella and/or nasal dorsum. (A-C) Hyaluronic acid-injected patients have skin necrosis. (D) Hyaluronic acid-injected patient, who were also treated with subcutaneous hyaluronidase injection showed mild erythema in the injected area. Autologous fat-injected patients also have (E) mild erythema or (F) normal appearance in the injected area. Case numbers are identical to those in Table 1.
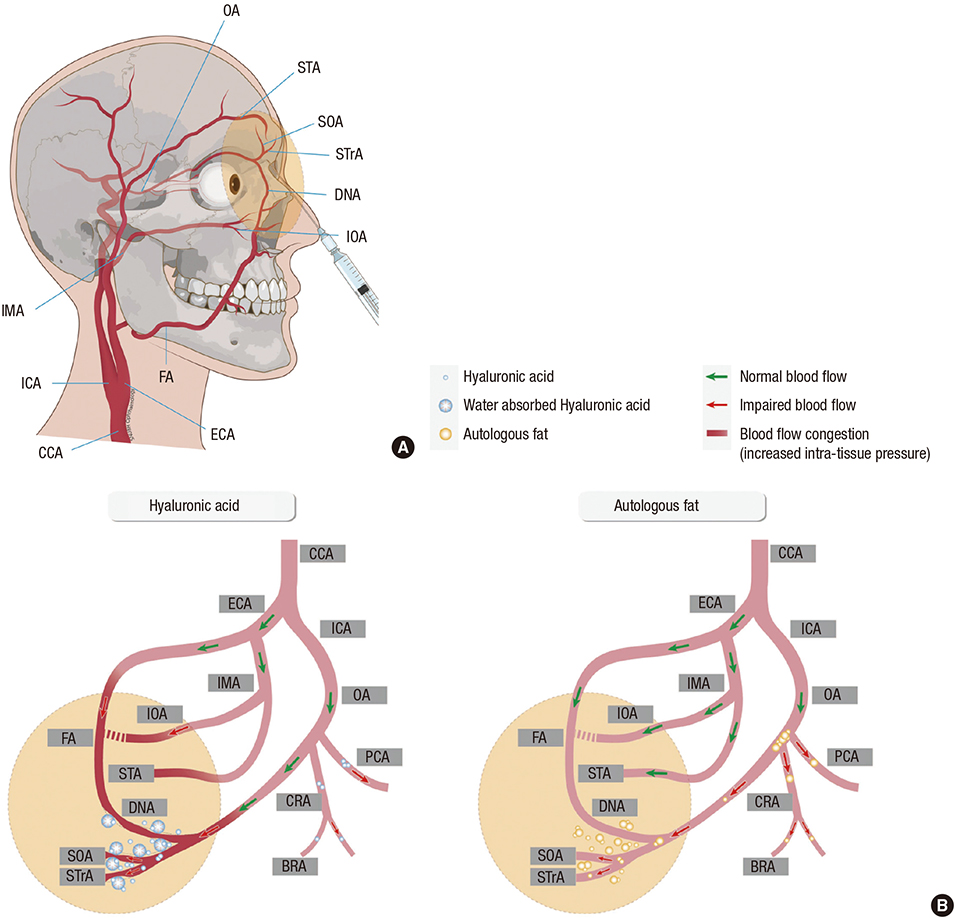
Fig. 6 Schematic drawing of vascular anatomy and the comparison of possible obstruction mechanism between hyaluronic acid and autologous fat. (A) Vascular anatomy of external and internal carotid artery and its ophthalmic and facial branches. (B) Hyaluronic acid (HA) molecules are small and uniform in size, compared to fat. HA may obstruct the central retinal artery, posterior ciliary arteries, and branch retinal arteries. In addition, the pressure gradient may be diminished between the ophthalmic artery and its distal ends because the distal intra-tissue pressure increases due to water absorption and volume expansion properties of HA, thereby decreasing blood flow. On the other hand, fat particles are composed of various sizes; thus, they can concomitantly obstruct from small arteries to the proximal part of the ophthalmic artery. Filler injected area and possible affected vascular area is drawn with yellow colored circle in A and B. BRA, branch retinal artery; CCA, common carotid artery; CRA, central retinal artery; DNA, dorsal nasal artery; ECA, external carotid artery; FA, facial artery; ICA, internal carotid artery; IMA, internal maxillary artery; IOA, infraorbital artery; OA, ophthalmic artery; PCA, posterior ciliary artery; SOA, supraorbital artery; STA, superficial temporal artery; STrA, supra-trochlear artery.
Reference
-
1. American Society of Plastic Surgeons. 2014 plastic surgery statistics report. accessed on 12 June 2015. Available at Http://www.Plasticsurgery.Org/news/plastic-surgery-statistics/2014-statistics.Html.2. Danesh-Meyer HV, Savino PJ, Sergott RC. Case reports and small case series: ocular and cerebral ischemia following facial injection of autologous fat. Arch Ophthalmol. 2001; 119:777–778.3. Park SH, Sun HJ, Choi KS. Sudden unilateral visual loss after autologous fat injection into the nasolabial fold. Clin Ophthalmol. 2008; 2:679–683.4. Sung MS, Kim HG, Woo KI, Kim YD. Ocular ischemia and ischemic oculomotor nerve palsy after vascular embolization of injectable calcium hydroxylapatite filler. Ophthal Plast Reconstr Surg. 2010; 26:289–291.5. Kim YJ, Kim SS, Song WK, Lee SY, Yoon JS. Ocular ischemia with hypotony after injection of hyaluronic acid gel. Ophthal Plast Reconstr Surg. 2011; 27:e152–e155.6. Park SJ, Woo SJ, Park KH, Hwang JM, Hwang GJ, Jung C, Kwon OK. Partial recovery after intraarterial pharmacomechanical thrombolysis in ophthalmic artery occlusion following nasal autologous fat injection. J Vasc Interv Radiol. 2011; 22:251–254.7. Lazzeri D, Agostini T, Figus M, Nardi M, Pantaloni M, Lazzeri S. Blindness following cosmetic injections of the face. Plast Reconstr Surg. 2012; 129:995–1012.8. Park SW, Woo SJ, Park KH, Huh JW, Jung C, Kwon OK. Iatrogenic retinal artery occlusion caused by cosmetic facial filler injections. Am J Ophthalmol. 2012; 154:653–662.e1.9. Oh BL, Jung C, Park KH, Hong YJ, Woo SJ. Therapeutic intra-arterial hyaluronidase infusion for ophthalmic artery occlusion following cosmetic facial filler (hyaluronic acid) injection. Neuroophthalmology. 2014; 38:39–43.10. Carle MV, Roe R, Novack R, Boyer DS. Cosmetic facial fillers and severe vision loss. JAMA Ophthalmol. 2014; 132:637–639.11. Kim YK, Ryoo NK, Park KH. Occlusion caused by cosmetic facial filler injection. JAMA Ophthalmol. 2015; 133:224–225.12. Park KH, Kim YK, Woo SJ, Kang SW, Lee WK, Choi KS, Kwak HW, Yoon IH, Huh K, Kim JW, et al. Iatrogenic occlusion of the ophthalmic artery after cosmetic facial filler injections: a national survey by the Korean Retina Society. JAMA Ophthalmol. 2014; 132:714–723.13. Grunebaum LD, Bogdan Allemann I, Dayan S, Mandy S, Baumann L. The risk of alar necrosis associated with dermal filler injection. Dermatol Surg. 2009; 35:1635–1640.14. Dayan SH, Arkins JP, Mathison CC. Management of impending necrosis associated with soft tissue filler injections. J Drugs Dermatol. 2011; 10:1007–1012.15. Kim JE, Sykes JM. Hyaluronic acid fillers: history and overview. Facial Plast Surg. 2011; 27:523–528.16. Humphrey S, Carruthers J, Carruthers A. Clinical experience with 11,460 mL of a 20-mg/mL, smooth, highly cohesive, viscous hyaluronic acid filler. Dermatol Surg. 2015; 41:1060–1067.17. Cox SE, Adigun CG. Complications of injectable fillers and neurotoxins. Dermatol Ther. 2011; 24:524–536.18. Cavallini M, Gazzola R, Metalla M, Vaienti L. The role of hyaluronidase in the treatment of complications from hyaluronic acid dermal fillers. Aesthet Surg J. 2013; 33:1167–1174.19. Hirsch RJ, Cohen JL, Carruthers JD. Successful management of an unusual presentation of impending necrosis following a hyaluronic acid injection embolus and a proposed algorithm for management with hyaluronidase. Dermatol Surg. 2007; 33:357–360.20. Kim DW, Yoon ES, Ji YH, Park SH, Lee BI, Dhong ES. Vascular complications of hyaluronic acid fillers and the role of hyaluronidase in management. J Plast Reconstr Aesthet Surg. 2011; 64:1590–1595.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multifocal Retinal and Ciliary Artery Occlusion with Submacular Hemorrhage Following Cosmetic Facial Filler Injection
- Incomplete Central Retinal Artery Occlusion
- Multiple Cerebral Infarctions with Neurological Symptoms and Ophthalmic Artery Occlusion after Filler Injection
- Successful Endovascular Thrombectomy in a Patient with Monocular Blindness Due to Thrombus of the Ophthalmic Artery Orifice
- A Case of Sudden Unilateral Visual Loss Following Injection of Filler into the Glabella
