Comparison of 3 and 7 Tesla Magnetic Resonance Imaging of Obstructive Hydrocephalus Caused by Tectal Glioma
- Affiliations
-
- 1Medical Neuroscience and Neurosurgery, Chungbuk National University Hospital, Cheongju, Korea. youngseokparkmd@gmail.com
- 2Bioimaging Research Team, Korea Basic Science Institute, Cheongju, Korea.
- 3Department of Bio-Analytical Science, Korea University of Science and Technology, Daejeon, Korea.
- 4Department of Neurosurgery, Chungbuk National University Hospital, Cheongju, Korea.
- KMID: 2356987
- DOI: http://doi.org/10.14791/btrt.2016.4.2.150
Abstract
- Obstructive hydrocephalus caused by tectal glioma, which relived by neuroendoscopy, have been described using 3.0 Tesla magnetic resonance imaging (3T MRI) so far, we present the results obtained from 3T and 7T MRI in this patient. A 21-year-old woman presented at our hospital with gait disturbance, hormonal insufficiency, and urinary incontinence that began prior to 6 years of age. 3.0T MRI revealed a non-enhancing tectal mass along with obstructive hydrocephalus. The mass measured approximately 1.1×1.0×1.2 cm. An endoscopic third ventriculostomy was performed to relieve the hydrocephalus. We compared hydrocephalus and cerebrospinal fluid (CSF) flow findings from 3T and 7T MRI, both preoperative and postoperative at 1, 6 months. Intraventricular CSF voiding on T2-weighted images obtained with 7T MRI showed greater fluid inversion than those obtained with 3T MRI. This study shows that 7T brain MRI can provide detailed information on hydrocephalus caused by tectal glioma. Further studies are needed to develop refined 7T MRI protocols for better images of hydrocephalus.
MeSH Terms
Figure
-

Fig. 1 Preoperative 3T MRI imaging. A: Axial T2-weighted 3T MR image confirming the presence of significant hydrocephalus. B: Axial T2-weighted 3T MR imaging confirming the tumor in the tectal plate. C: Axial T1-weighted gadolinium enhance 3T MR imaging confirming the presence of significant hydrocephalus. D: Axial T1-weighted gadolinium enhance 3T MR imaging confirming the the tumor in the tectal plate. E: Coronal T1-weighted gadolinium enhance 3T MR imaging. F: Sagittal T1-weighted 3T MR imaging hydrocephalus with non enhancing mass.

Fig. 2 Preoperative 7T MR axial T2-weighted image with hydrocephalus (A), axial T2-weighted image showing tectal glioma (B), and sagittal T1-weighted image (C). Postoperative 6 month MRI imaging (D-F). The arrow showing tectal glioma.
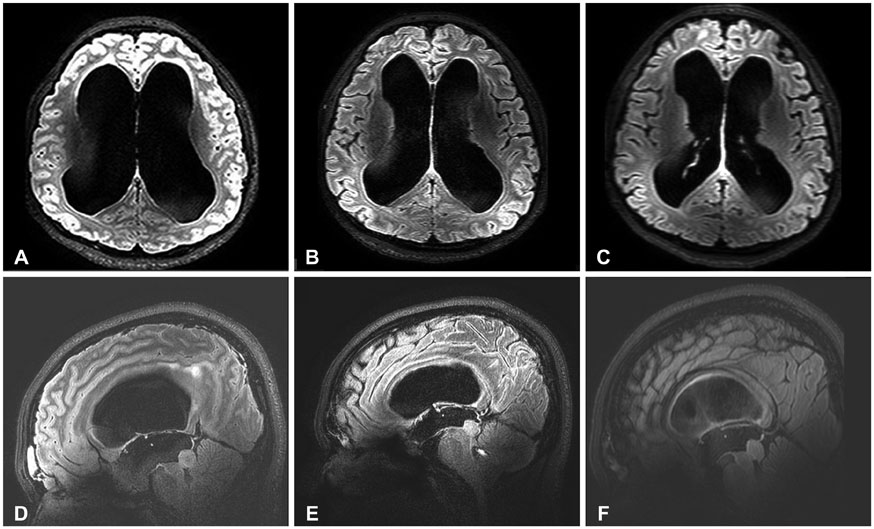
Fig. 3 Preopeartive imaging (A and D) and postoperative 1 month (B and E), postop 6 month 7T (C and F) fluid attenuation inversion recovery (FLAIR) MR studies showing parenchymal change and ventricle size. Preoperative (D) and postoperative (E and F) sagittal FLAIR MR image demonstrating a decrease in the ventricle scalloping and stable appearance of the tectal glioma.

Fig. 4 Preoperative sagittal T1-weighted gadolinium enhanced 3T MR (A), 7T MR (B), and postoperative 7T fluid attenuation inversion recovery MRI image (C). The arrow show floor of third ventricle, this membrane better delineated in 7T MRI image, also tectal glioma showing more prominent in 7T MRI (arrowhead).
Reference
-
1. Li KW, Roonprapunt C, Lawson HC, et al. Endoscopic third ventriculostomy for hydrocephalus associated with tectal gliomas. Neurosurg Focus. 2005; 18(6A):E2.
Article2. Lupo JM, Banerjee S, Hammond KE, et al. GRAPPA-based susceptibility-weighted imaging of normal volunteers and patients with brain tumor at 7 T. Magn Reson Imaging. 2009; 27:480–488.
Article3. Moenninghoff C, Maderwald S, Theysohn JM, et al. Imaging of adult astrocytic brain tumours with 7 T MRI: preliminary results. Eur Radiol. 2010; 20:704–713.
Article4. Cho ZH, Kang CK, Han JY, et al. Observation of the lenticulostriate arteries in the human brain in vivo using 7.0T MR angiography. Stroke. 2008; 39:1604–1606.
Article5. Dashner RA, Kangarlu A, Clark DL, RayChaudhury A, Chakeres DW. Limits of 8-Tesla magnetic resonance imaging spatial resolution of the deoxygenated cerebral microvasculature. J Magn Reson Imaging. 2004; 19:303–307.
Article6. Paek SL, Chung YS, Paek SH, et al. Early experience of pre- and post-contrast 7.0T MRI in brain tumors. J Korean Med Sci. 2013; 28:1362–1372.
Article7. Chen G, Zheng J, Xiao Q, Liu Y. Application of phase-contrast cine magnetic resonance imaging in endoscopic aqueductoplasty. Exp Ther Med. 2013; 5:1643–1648.
Article8. Akay R, Kamisli O, Kahraman A, Oner S, Tecellioglu M. Evaluation of aqueductal CSF flow dynamics with phase contrast cine MR imaging in idiopathic intracranial hypertension patients: preliminary results. Eur Rev Med Pharmacol Sci. 2015; 19:3475–3479.9. Forner Giner J, Sanz-Requena R, Flórez N, et al. Quantitative phase-contrast MRI study of cerebrospinal fluid flow: a method for identifying patients with normal-pressure hydrocephalus. Neurologia. 2014; 29:68–75.
Article10. Fin L, Grebe R. Three dimensional modeling of the cerebrospinal fluid dynamics and brain interactions in the aqueduct of sylvius. Comput Methods Biomech Biomed Engin. 2003; 6:163–170.
Article11. Conner M, Gillespie J, Schiff E, Holmes D, Frey M, Quick S. Experimental infection of horses and ponies by oral and intranasal routes with New York State reovirus type 3 and German reovirus types 1 and 3 equine isolates. Zentralbl Veterinarmed B. 1984; 31:707–717.
Article12. Conner ES, Foley L, Black PM. Experimental normal-pressure hydrocephalus is accompanied by increased transmantle pressure. J Neurosurg. 1984; 61:322–327.
Article13. Schroeder HW, Schweim C, Schweim KH, Gaab MR. Analysis of aqueductal cerebrospinal fluid flow after endoscopic aqueductoplasty by using cine phase-contrast magnetic resonance imaging. J Neurosurg. 2000; 93:237–244.
Article14. Hayashi N, Matsumae M, Yatsushiro S, Hirayama A, Abdullah A, Kuroda K. Quantitative analysis of cerebrospinal fluid pressure gradients in healthy volunteers and patients with normal pressure hydrocephalus. Neurol Med Chir (Tokyo). 2015; 55:657–662.
Article15. Yatsushiro S, Hirayama A, Matsumae M, Kuroda K. Visualization of pulsatile CSF motion separated by membrane-like structure based on four-dimensional phase-contrast (4D-PC) velocity mapping. Conf Proc IEEE Eng Med Biol Soc. 2013; 2013:6470–6473.
Article16. Tallantyre EC, Morgan PS, Dixon JE, et al. A comparison of 3T and 7T in the detection of small parenchymal veins within MS lesions. Invest Radiol. 2009; 44:491–494.
Article17. Schmitt F, Grosu D, Mohr C, et al. [3 Tesla MRI: successful results with higher field strengths]. Radiologe. 2004; 44:31–47.18. Feinberg DA, Mark AS. Human brain motion and cerebrospinal fluid circulation demonstrated with MR velocity imaging. Radiology. 1987; 163:793–799.
Article19. Stucht D, Danishad KA, Schulze P, Godenschweger F, Zaitsev M, Speck O. Highest resolution in vivo human brain MRI using prospective motion correction. PLoS One. 2015; 10:e0133921.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tectal glioma presenting with adult-onset epileptic seizures
- A Neonatal Form of Alexander Disease Presented with Intractable Seizures and Obstructive Hydrocephalus
- High field strength magnetic resonance imaging of cardiovascular diseases
- A comparison between obstructive hydrocephalus and non-obstructive hydrocephalus on midsagittal brain MRI
- Introduction to high field strength magnetic resonance imaging
