A Stable Secondary Gliosarcoma with Extensive Systemic Metastases: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, Kwangju Christian Hospital, Gwangju, Korea.
- 2Department of Neurosurgery, Chonnam National University Hwasun Hospital & Medical School, Gwangju, Korea. jung-ty@chonnam.ac.kr
- 3Department of Pathology, Chonnam National University Research Institute of Medical Sciences, Chonnam National University Hwasun Hospital & Medical School, Gwangju, Korea.
- KMID: 2356983
- DOI: http://doi.org/10.14791/btrt.2016.4.2.133
Abstract
- A 63-year-old man complained of intermittent motor weakness of his arm. The magnetic resonance image (MRI) of his brain displayed a high signal lesion in right cingulate gyrus on T2 weighted image. One year later, he showed a stuporous mental status with repeated seizures, and the follow-up brain MRI showed heterogeneously enhanced mass associated with bleeding. He was treated with surgery and radiotherapy for secondary glioblastomas in right cingulate gyrus. One year more later, a mass recurred on the left frontal base, and gliosarcoma was diagnosed. After tumor resection, ventriculoperitoneal shunt, chemotherapy, and re-radiation therapy, all brain lesions were stable. Fourteen months after the diagnosis of gliosarcoma, he complained of dyspnea and back pain. Torso positron emission tomography/computed tomography revealed multiple metastatic lesions in both lungs, pericardium, pleura, liver, lymph nodes, and bones, and metastatic gliosarcoma was diagnosed. One month later, the patient died because of the systemic metastases. We present an unusual case of secondary gliosarcoma with stable brain lesions and extensive systemic metastases.
MeSH Terms
Figure
-
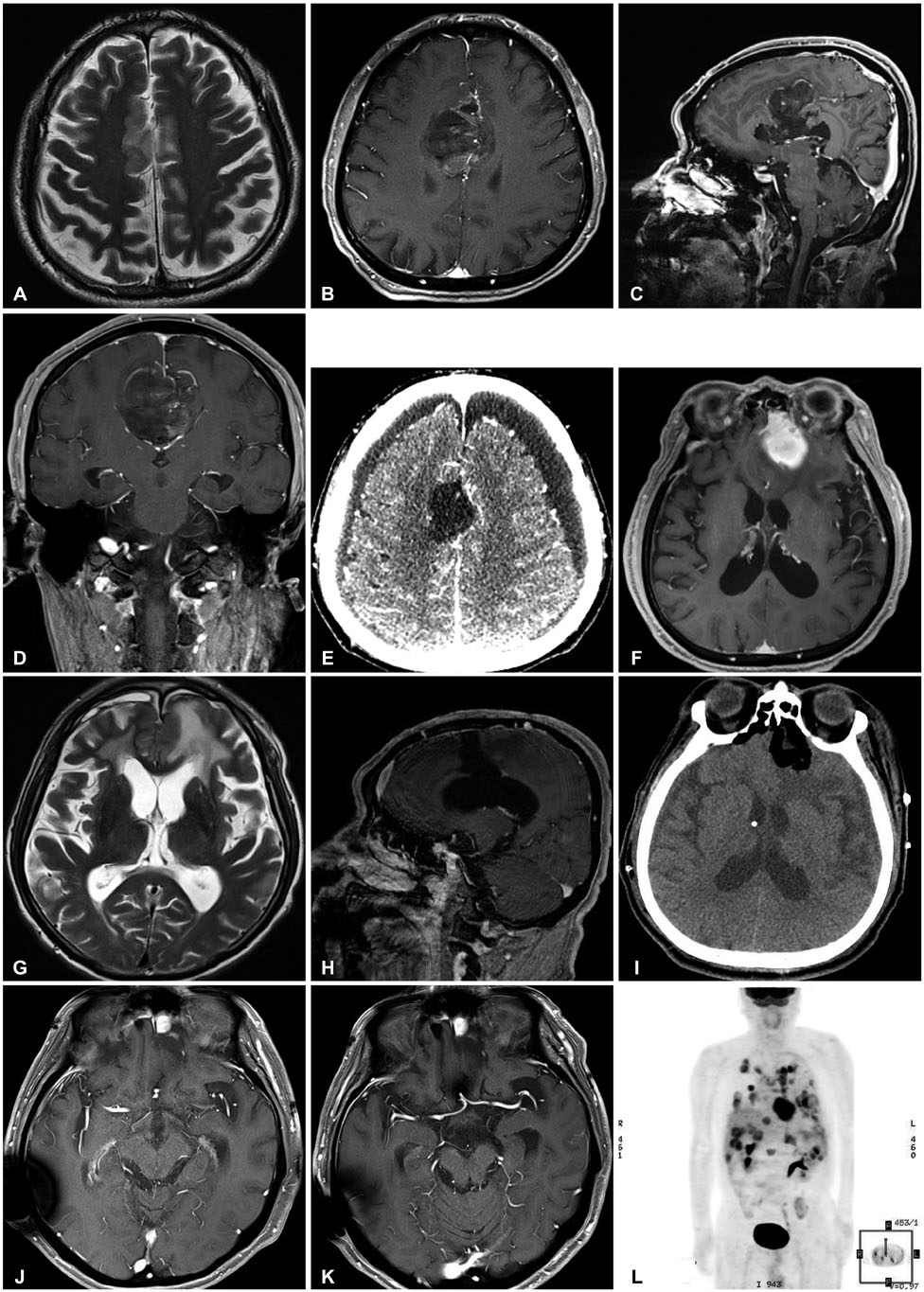
Fig. 1 Radiologic findings of glioblastoma and gliosarcoma. A: Initial T2-weighted magnetic resonance images (MRI) of the brain displays a high-signal lesion in right cingulate gyru. B, C, and D: One year later, follow-up MRI shows a heterogeneously enhanced mass associated with bleeding in right cingulate gyrus on axial (B), sagittal (C), and coronal (D) images of enhanced T1-weighted image. E: On brain computed tomography (CT), the tumor was totally resected. F: Brain MRI shows a homogenous enhanced lesion in the left frontal base on axial view of enhanced T1-weighted image. G: Ventricular enlargement with periventricular lucency was shown on T2-weighted MR image. H: There was no recurred lesion of right cingulate gyrus on enhanced T1-weighted sagittal image. I: Brain CT shows that the mass was totally resected, and a ventriculoperitoneal shunt was placed. J: After surgery and chemotherapy, the mass of left frontal base was recurred on axial view of enhanced T1-weighted image. K: After radiotherapy, the mass of left frontal base was stable on axial view of enhanced T1-weighted image. L: Torso positron emission tomography/CT shows multiple metastatic lesions in both the lungs, pericardium, left pleura, right mediastinal pleura, liver, lymph nodes, and bones.
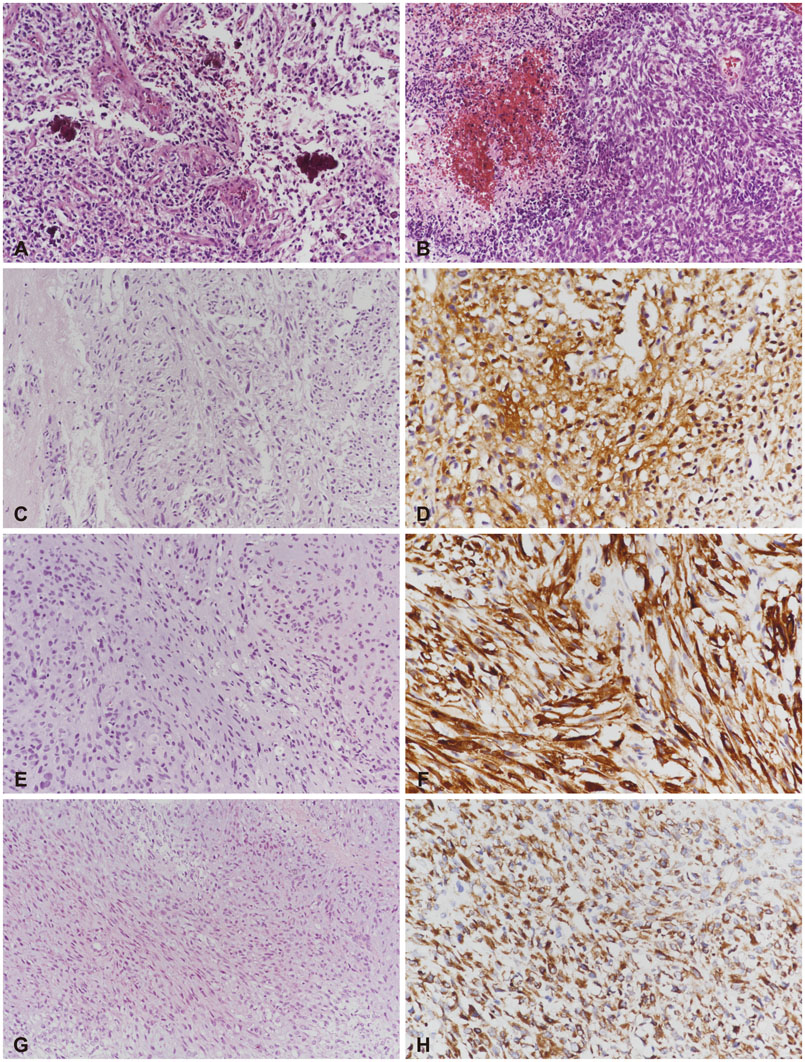
Fig. 2 Pathologic findings of glioblastoma and gliosarcoma within brain and liver. Glioblastoma of brain; pleomorphic neoplastic cells with endothelial proliferation (A) and pseudopalisading necrosis (B) (original magnification, ×100; hematoxylin and eosin staining). Gliosarcoma of brain; the glial component of pleomorphic astrocytic cells (C, original magnification, ×100; hematoxylin and eosin staining), immunopositivity for glial fibrillary acidic protein (D, original magnification, ×200), sarcomatous component of spindle cells (E, original magnification, ×100; hematoxylin and eosin staining) and immunopositivity for nestin (F, original magnification, ×200). Gliosarcoma of liver; sarcomatous component of spindle cells (G, original magnification, ×100; hematoxylin and eosin staining) and immunopositivity for nestin (H, original magnification, ×200).
Reference
-
1. Ben Nsir A, Thai QA, Kassar AZ, Ben Said I, Jemel H. Primary cerebellar gliosarcoma with extracranial metastases: an orphan differential diagnosis. World Neurosurg. 2015; 84:2076.e13-7.
Article2. Rapp M, Felsberg J, Sorg RV, Gerharz CD, Sabel M. Case report: extracranial metastasis from gliosarcoma--the influence of immune system. Br J Neurosurg. 2011; 25:286–288.
Article3. Andaloussi-Saghir K, Oukabli M, El Marjany M, Sifat H, Hadadi K, Mansouri H. Secondary gliosarcoma after the treatment of primary glioblastoma multiforme. N Am J Med Sci. 2011; 3:527–530.
Article4. Rizvi S, Asghar AH, Mehboob J. Gliosarcoma: a rare variant of glioblastoma multiforme. J Pak Med Assoc. 2010; 60:773–775.5. Mason A, Villavicencio AT, Nelson EL, Forsythe RC, Burneikiene S. Post-treatment gliosarcoma extension into the pterygomaxillary fossa: literature review and case report. Cureus. 2016; 8:e700.
Article6. Dawar R, Fabiano AJ, Qiu J, Khushalani NI. Secondary gliosarcoma with extra-cranial metastases: a report and review of the literature. Clin Neurol Neurosurg. 2013; 115:375–380.
Article7. Lun M, Lok E, Gautam S, Wu E, Wong ET. The natural history of extracranial metastasis from glioblastoma multiforme. J Neurooncol. 2011; 105:261–273.
Article
