Therapeutic Strategy for Cavernous Sinus-Invading Non-Functioning Pituitary Adenomas Based on the Modified Knosp Grading System
- Affiliations
-
- 1Department of Neurosurgery, Endoscopic Skull Base Surgery Clinic, Brain Tumor Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. neurokong@gmail.com petit919@naver.com
- KMID: 2356972
- DOI: http://doi.org/10.14791/btrt.2016.4.2.63
Abstract
- BACKGROUND
Non-functioning pituitary adenomas (NFPA) invading into the cavernous sinus are surgically challenging. To decrease recurrence rate, surgeon makes a strong endeavor to resect tumor gross totally. However, gross total resection (GTR) is difficult to achieve with cavernous sinus invasion. Recently, a new classification system for cavernous invasion of pituitary adenomas was suggested. The aim of this study is to validate this new classification system and to identify limitations and considerations in designing treatment strategies for patients with NFPA involving the cavernous sinus.
METHODS
Between January 2000 and January 2012, 275 patients who underwent operation for NFPA were enrolled in the study. Median age was 50 years (15-79 years). There were 145 males and 130 females. The median follow-up duration was 4 years (range 1-12.5 years).
RESULTS
Related to extent of tumor removal, GTR was obtained in 184 patients (66.9%), near total resection (NTR) was obtained in 45 patients (16.3%), and sub-total resection (STR) was obtained in 46 patients (16.7%) of a total 275 patients. There were statistically significant differences between the extent of resection and the new Knosp classification (p<0.001). In the high-grade group of the new Knosp classification, there was no difference in recurrence between patients who underwent GTR or NTR only and those who underwent STR with adjuvant radiation therapy (p=0.515).
CONCLUSION
In case of high risk of surgical complications, STR with adjuvant radiation therapy can be considered as an alternative strategy for safe treatment of cavernous-invading adenomas.
MeSH Terms
Figure
-

Fig. 1 Kaplan-Meier survival curve according to the new Knosp classification system.
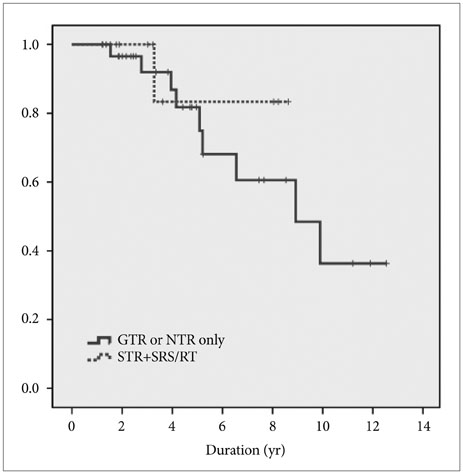
Fig. 2 Kaplan-Meier survival curve between GTR or NTR only and STR with SRS/RT in high-grade new Knosp classification (grade 3A, 3B, and 4) disease. GTR, gross total resection; STR, subtotal resection; NTR, near total resection; SRS, stereotactic radiosurgery; RT, radiotherapy.
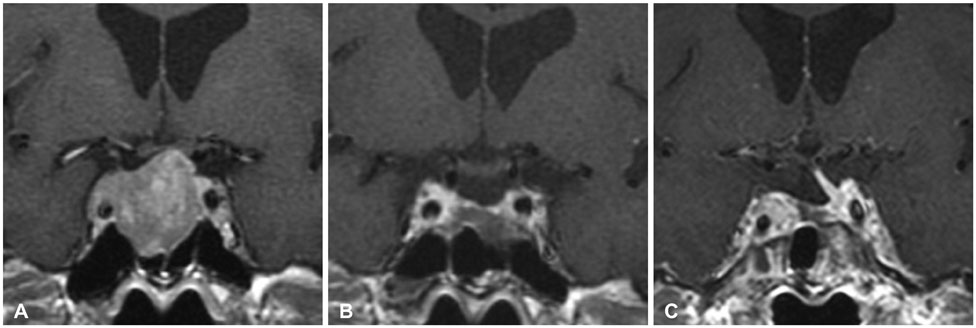
Fig. 3 A Knosp grade 3A macroadenoma in a 61-year-old man. A: Preoperative image revealing the tumor extending into cavernous sinus. B: Postoperative image showing gross total resection. C: Without any adjuvant treatment, the tumor was recurred 4 years after the operation.

Fig. 4 A Knosp grade 4 macroadenoma in a 44-year-old man. A: Preoperative image showing marked extension of tumor to supra sellar and cavernous sinus. B: Postoperative image showing residual tumor to receive a radiation therapy. C: No significant change 9 years after the operation.
Reference
-
1. Krayenbühl N, Hafez A, Hernesniemi JA, Krisht AF. Taming the cavernous sinus: technique of hemostasis using fibrin glue. Neurosurgery. 2007; 61:3 Suppl. E52. discussion E52.
Article2. DeMonte F, Smith HK, al-Mefty O. Outcome of aggressive removal of cavernous sinus meningiomas. J Neurosurg. 1994; 81:245–251.
Article3. Chang EF, Zada G, Kim S, et al. Long-term recurrence and mortality after surgery and adjuvant radiotherapy for nonfunctional pituitary adenomas. J Neurosurg. 2008; 108:736–745.
Article4. Brada M, Rajan B, Traish D, et al. The long-term efficacy of conservative surgery and radiotherapy in the control of pituitary adenomas. Clin Endocrinol (Oxf). 1993; 38:571–578.
Article5. Gittoes NJ, Bates AS, Tse W, et al. Radiotherapy for non-function pituitary tumours. Clin Endocrinol (Oxf). 1998; 48:331–337.6. Lillehei KO, Kirschman DL, Kleinschmidt-DeMasters BK, Ridgway EC. Reassessment of the role of radiation therapy in the treatment of endocrine-inactive pituitary macroadenomas. Neurosurgery. 1998; 43:432–438. discussion 438-9.
Article7. McCollough WM, Marcus RB Jr, Rhoton AL Jr, Ballinger WE, Million RR. Long-term follow-up of radiotherapy for pituitary adenoma: the absence of late recurrence after greater than or equal to 4500 cGy. Int J Radiat Oncol Biol Phys. 1991; 21:607–614.
Article8. Knosp E, Steiner E, Kitz K, Matula C. Pituitary adenomas with invasion of the cavernous sinus space: a magnetic resonance imaging classification compared with surgical findings. Neurosurgery. 1993; 33:610–617. discussion 617-8.
Article9. Vieira JO Jr, Cukiert A, Liberman B. Evaluation of magnetic resonance imaging criteria for cavernous sinus invasion in patients with pituitary adenomas: logistic regression analysis and correlation with surgical findings. Surg Neurol. 2006; 65:130–135. discussion 135.
Article10. Woodworth GF, Patel KS, Shin B, et al. Surgical outcomes using a medial-to-lateral endonasal endoscopic approach to pituitary adenomas invading the cavernous sinus. J Neurosurg. 2014; 120:1086–1094.
Article11. Zhao B, Wei YK, Li GL, et al. Extended transsphenoidal approach for pituitary adenomas invading the anterior cranial base, cavernous sinus, and clivus: a single-center experience with 126 consecutive cases. J Neurosurg. 2010; 112:108–117.
Article12. Nishioka H, Fukuhara N, Horiguchi K, Yamada S. Aggressive transsphenoidal resection of tumors invading the cavernous sinus in patients with acromegaly: predictive factors, strategies, and outcomes. J Neurosurg. 2014; 121:505–510.
Article13. Micko AS, Wöhrer A, Wolfsberger S, Knosp E. Invasion of the cavernous sinus space in pituitary adenomas: endoscopic verification and its correlation with an MRI-based classification. J Neurosurg. 2015; 122:803–811.
Article14. Ceylan S, Anik I, Koc K. A new endoscopic surgical classification and invasion criteria for pituitary adenomas involving the cavernous sinus. Turk Neurosurg. 2011; 21:330–339.
Article15. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977; 33:159–174.
Article16. Ceylan S, Koc K, Anik I. Endoscopic endonasal transsphenoidal approach for pituitary adenomas invading the cavernous sinus. J Neurosurg. 2010; 112:99–107.
Article17. Taussky P, Kalra R, Coppens J, Mohebali J, Jensen R, Couldwell WT. Endocrinological outcome after pituitary transposition (hypophysopexy) and adjuvant radiotherapy for tumors involving the cavernous sinus. J Neurosurg. 2011; 115:55–62.
Article18. Juraschka K, Khan OH, Godoy BL, et al. Endoscopic endonasal transsphenoidal approach to large and giant pituitary adenomas: institutional experience and predictors of extent of resection. J Neurosurg. 2014; 121:75–83.
Article19. Sheehan JP, Kondziolka D, Flickinger J, Lunsford LD. Radiosurgery for residual or recurrent nonfunctioning pituitary adenoma. J Neurosurg. 2002; 97:5 Suppl. 408–414.
Article20. Lee MH, Lee JH, Seol HJ, et al. Clinical concerns about recurrence of non-functioning pituitary adenoma. Brain Tumor Res Treat. 2016; 4:1–7.
Article21. Greenman Y, Ouaknine G, Veshchev I, Reider-Groswasser II, Segev Y, Stern N. Postoperative surveillance of clinically nonfunctioning pituitary macroadenomas: markers of tumour quiescence and regrowth. Clin Endocrinol (Oxf). 2003; 58:763–769.
Article22. Bradley KM, Adams CB, Potter CP, Wheeler DW, Anslow PJ, Burke CW. An audit of selected patients with non-functioning pituitary adenoma treated by transsphenoidal surgery without irradiation. Clin Endocrinol (Oxf). 1994; 41:655–659.
Article23. Ciric I, Ragin A, Baumgartner C, Pierce D. Complications of transsphenoidal surgery: results of a national survey, review of the literature, and personal experience. Neurosurgery. 1997; 40:225–236. discussion 236-7.
Article24. Park P, Chandler WF, Barkan AL, et al. The role of radiation therapy after surgical resection of nonfunctional pituitary macroadenomas. Neurosurgery. 2004; 55:100–106. discussion 106-7.
Article25. Turner HE, Stratton IM, Byrne JV, Adams CB, Wass JA. Audit of selected patients with nonfunctioning pituitary adenomas treated without irradiation - a follow-up study. Clin Endocrinol (Oxf). 1999; 51:281–284.
Article26. Flickinger JC, Nelson PB, Martinez AJ, Deutsch M, Taylor F. Radiotherapy of nonfunctional adenomas of the pituitary gland. Results with long-term follow-up. Cancer. 1989; 63:2409–2414.
Article27. Gittoes NJ. Radiotherapy for non-functioning pituitary tumors--when and under what circumstances? Pituitary. 2003; 6:103–108.
Article28. Cottier JP, Destrieux C, Brunereau L, et al. Cavernous sinus invasion by pituitary adenoma: MR imaging. Radiology. 2000; 215:463–469.
Article29. Dickerman RD, Oldfield EH. Basis of persistent and recurrent Cushing disease: an analysis of findings at repeated pituitary surgery. J Neurosurg. 2002; 97:1343–1349.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Parasellar Extension Grades and Surgical Extent in Endoscopic Endonasal Transsphenoidal Surgery for Pituitary Adenomas : A Single Surgeon's Consecutive Series with the Aspects of Reliability and Clinical Validity
- Management of Tumors Involving the Cavernous Sinus: Experience of 10 Cases
- Surgical Results of Growth Hormone-Secreting Pituitary Adenoma
- Association of PTTG1 expression with invasiveness of non-functioning pituitary adenomas
- Epidemiology of Functioning Pituitary Adenomas
