J Rheum Dis.
2016 Oct;23(5):332-335. 10.4078/jrd.2016.23.5.332.
Serotonin Syndrome following Duloxetine Administration in a Fibromyalgia Patient: Case Report and Literature Review
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Maryknoll Medical Center, Busan, Korea. ete@lycos.co.kr
- 2Department of Neurology, Maryknoll Medical Center, Busan, Korea.
- KMID: 2356490
- DOI: http://doi.org/10.4078/jrd.2016.23.5.332
Abstract
- Serotonin syndrome, an adverse drug reaction, is a consequence of excess serotonergic agonism of central nervous system receptors and peripheral serotonergic receptors. Serotonin syndrome has been associated with large numbers of drugs and drug combinations, and serotonin-norepinephrine reuptake inhibitor-induced serotonin syndrome is rare. It is often described as a sign of excess serotonin ranging from tremor in mild cases to delirium, neuromuscular rigidity, and hyperthermia in life-threatening cases. Diagnosis is based on the symptoms and patient's history, and several diagnostic criteria have been developed. We experienced a rare case of fibromyalgia accompanied by tremor, hyperreflexia, spontaneous clonus, muscle rigidity, and diaphoresis after 10 days of single use of duloxetine 30 mg. Only one case of serotonin syndrome resulting from administration of duloxetine has been reported in Korea, however that case resulted from co-administration of fluoxetine. We report here on this case along with a review of the relevant literature.
Keyword
MeSH Terms
-
Central Nervous System
Delirium
Diagnosis
Drug Combinations
Drug-Related Side Effects and Adverse Reactions
Duloxetine Hydrochloride*
Felodipine
Fever
Fibromyalgia*
Fluoxetine
Humans
Korea
Muscle Rigidity
Reflex, Abnormal
Serotonin Syndrome*
Serotonin*
Tremor
Drug Combinations
Duloxetine Hydrochloride
Felodipine
Fluoxetine
Serotonin
Figure
-

Figure 1. 18-channel electroen-cephalogram with electrocardio-graphy (ECG) monitoring performed with a patient in awake to drowsy state. EOG: electrooculo-graphy.
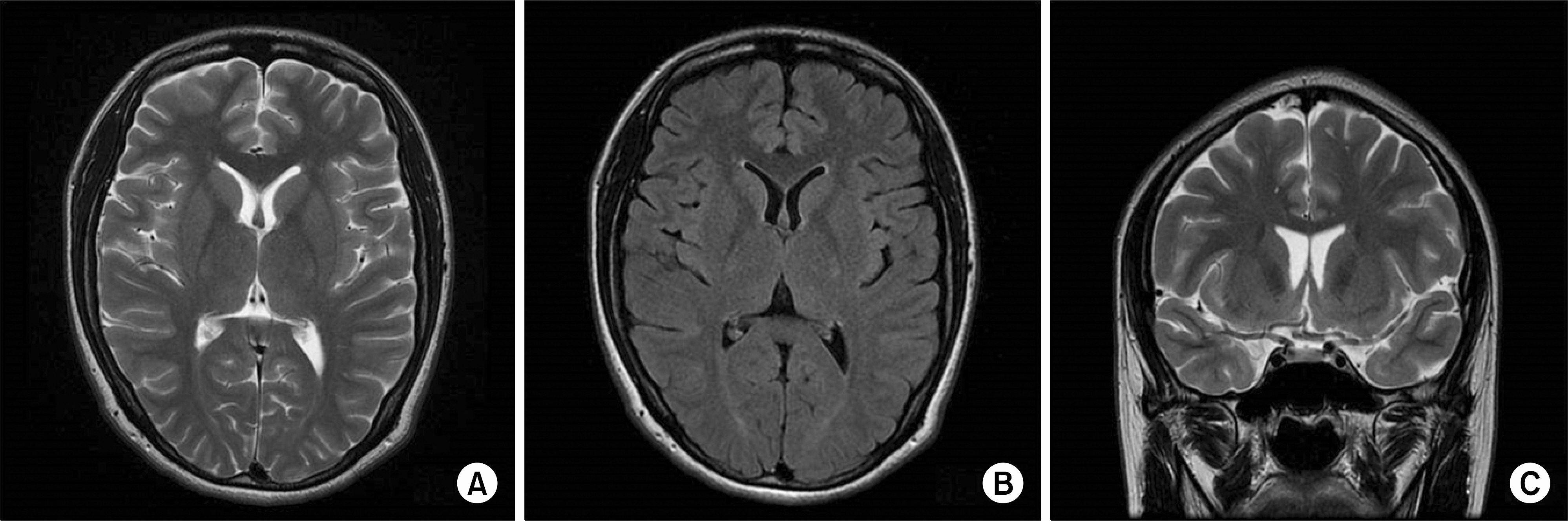
Figure 2. Brain magnetic resonance imaging (MRI). (A) Axial T2-weighted MRI. (B) Axial FLAIR MRI. (C) Coronal T2-weighted MRI.
Reference
-
1. Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005; 352:1112–20.
Article2. Gaffney RR, Schreibman IR. Serotonin syndrome in a patient on trazodone and duloxetine who received fentanyl following a percutaneous liver biopsy. Case Rep Gastroenterol. 2015; 9:132–6.
Article3. Gollapudy S, Kumar V, Dhamee MS. A case of serotonin syndrome precipitated by fentanyl and ondansetron in a patient receiving paroxetine, duloxetine, and bupropion. J Clin Anesth. 2012; 24:251–2.
Article4. Gelener P, Gorgulu U, Kutlu G, Ucler S, Inan LE. Serotonin syndrome due to duloxetine. Clin Neuropharmacol. 2011; 34:127–8.
Article5. You S, Noh JS. A case of serotonin syndrome induced by fluoxetine and duloxetine independently in a same patient. Korean J Psychopharmacol. 2012; 23:74–7.6. Gnanadesigan N, Espinoza RT, Smith R, Israel M, Reuben DB. Interaction of serotonergic antidepressants and opioid analgesics: Is serotonin syndrome going undetected? J Am Med Dir Assoc. 2005; 6:265–9.
Article7. Nisijima K, Shioda K, Yoshino T, Takano K, Kato S. Memantine, an NMDA antagonist, prevents the development of hyperthermia in an animal model for serotonin syndrome. Pharmacopsychiatry. 2004; 37:57–62.
Article8. Gillman PK. A review of serotonin toxicity data: implications for the mechanisms of antidepressant drug action. Biol Psychiatry. 2006; 59:1046–51.
Article9. Lamberg JJ, Gordin VN. Serotonin syndrome in a patient with chronic pain polypharmacy. Pain Med. 2014; 15:1429–31.10. Dunkley EJ, Isbister GK, Sibbritt D, Dawson AH, Whyte IM. The hunter serotonin toxicity criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM. 2003; 96:635–42.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Serotonin Syndrome Induced by Fluoxetine and Duloxetine Independently in a Same Patient
- Two Cases of Hyponatremia Induced by Duloxetine for Treating Peripheral Neuropathic Pain
- Diagnosis and Treatment of Fibromyalgia Syndrome
- A Case of Postural Orthostatic Tachycardia Syndrome Associated with Migraine and Fibromyalgia
- Implantable drug delivery systems with morphine in fibromyalgia: A case report
