Clinical outcomes of subtotal cholecystectomy performed for difficult cholecystectomy
- Affiliations
-
- 1Department of Surgery, Chosun University School of Medicine, Gwangju, Korea. spmun@chosun.ac.kr
- KMID: 2356372
- DOI: http://doi.org/10.4174/astr.2016.91.5.226
Abstract
- PURPOSE
Laparoscopic subtotal cholecystectomy (LSC) can be an alternative surgical technique for difficult cholecystectomies. Surgeons performing LSC sometimes leave the posterior wall of the gallbladder (GB) to shorten the operation time and avoid liver injury. However, leaving the inflamed posterior GB wall is a major concern. In this study, we evaluated the clinical outcomes of standard laparoscopic cholecystectomy (SLC), LSC, and LSC removing only anterior wall of the GB (LSCA).
METHODS
We retrospectively reviewed the medical records of laparoscopic cholecystectomies performed between January 2006 to December 2015 and analyzed the outcomes of SLC, LSC, and LSCA.
RESULTS
A total of 1,037 patients underwent SLC. 22 patients underwent LSC; and 27 patients underwent LSCA. The mean operating times of SLC, LSC, and LSCA were 41, 74, and 68 minutes, respectively (P < 0.01). Blood loss was 5, 45, and 33 mL (P < 0.05). The mean lengths of postoperative hospitalization were 3.4, 5.4, and 5.8 days. Complications occurred in 24 SLC patients (2.3%), 2 LSC patients (9%), and 1 LSCA patient (3.7%). There was no mortality among the LSC and LSCA patients.
CONCLUSION
LSC and LSCA are safe and feasible alternatives for difficult cholecystectomies. These procedures help surgeons avoid bile duct injury and conversion to laparotomy. LSCA has the benefits of shorter operation time and less bleeding compared to LSC.
MeSH Terms
Figure
-
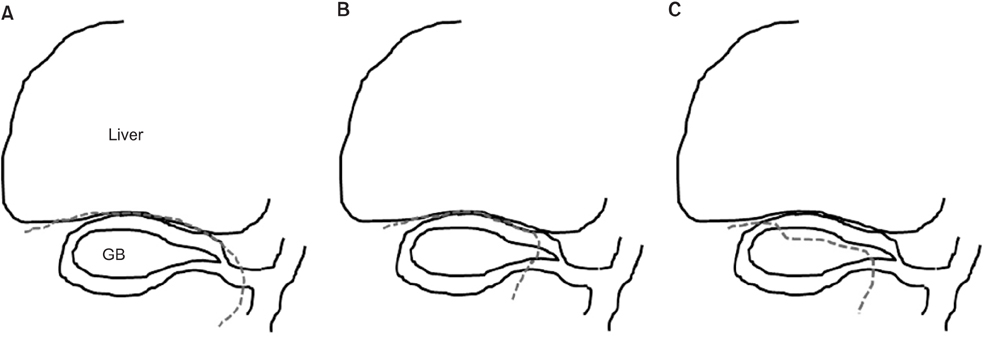
Fig. 1 Transection planes in SLC (A), LSC (B), and LSCA (C). (A) In SLC, the cystic duct is exposed and transected. The dissection is then made between the gallbladder and the liver. (B) In LSC, the transection is made at the level of the neck or body of the GB. The dissection is then made between the GB and the liver. The GB stump is sutured or packed with fibrin sealant. (C) In LSCA, the transection is made at the level of the neck or body of the GB. Without GB dissection, the anterior wall of the GB is transected with electrocautery or ultrasonic scissors. The GB stump is then sutured or packed with fibrin sealant. SLC, standard laparoscopic cholecystectomy; GB, gallbladder; LSC, laparoscopic subtotal cholecystectomy; LSCA, laparoscopic subtotal cholecystectomy removing the anterior wall of the GB.
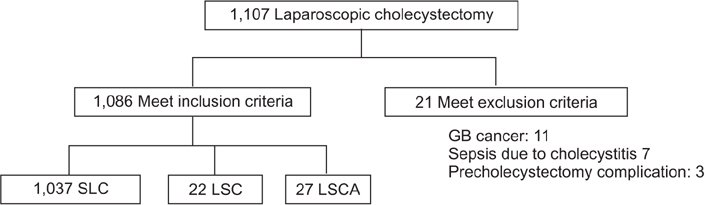
Fig. 2 Diagram of patients enrolled. GB, gallbladder; SLC, standard laparoscopic cholecystectomy; LSC, laparoscopic subtotal cholecystectomy; LSCA, laparoscopic subtotal cholecystectomy removing the anterior wall of the GB.
Reference
-
1. Khan TF. Modified subtotal cholecystectomy: a procedure for the difficult gall bladder. Med J Malaysia. 1992; 47:65–68.2. Zhong H, Gong JP. Mirizzi syndrome: experience in diagnosis and treatment of 25 cases. Am Surg. 2012; 78:61–65.3. Kaplan D, Inaba K, Chouliaras K, Low GM, Benjamin E, Lam L, et al. Subtotal cholecystectomy and open total cholecystectomy: alternatives in complicated cholecystitis. Am Surg. 2014; 80:953–955.4. Bornman PC, Terblanche J. Subtotal cholecystectomy: for the difficult gallbladder in portal hypertension and cholecystitis. Surgery. 1985; 98:1–6.5. Strasberg SM, Pucci MJ, Brunt LM, Deziel DJ. Subtotal cholecystectomy-"fenestrating" vs "reconstituting" subtypes and the prevention of bile duct injury: definition of the optimal procedure in difficult operative conditions. J Am Coll Surg. 2016; 222:89–96.6. Bickel A, Shtamler B. Laparoscopic subtotal cholecystectomy. J Laparoendosc Surg. 1993; 3:365–367.7. Elshaer M, Gravante G, Thomas K, Sorge R, Al-Hamali S, Ebdewi H. Subtotal cholecystectomy for "difficult gallbladders": systematic review and meta-analysis. JAMA Surg. 2015; 150:159–168.8. Michalowski K, Bornman PC, Krige JE, Gallagher PJ, Terblanche J. Laparoscopic subtotal cholecystectomy in patients with complicated acute cholecystitis or fibrosis. Br J Surg. 1998; 85:904–906.9. Sinha I, Smith ML, Safranek P, Dehn T, Booth M. Laparoscopic subtotal cholecystectomy without cystic duct ligation. Br J Surg. 2007; 94:1527–1529.10. Philips JA, Lawes DA, Cook AJ, Arulampalam TH, Zaborsky A, Menzies D, et al. The use of laparoscopic subtotal cholecystectomy for complicated cholelithiasis. Surg Endosc. 2008; 22:1697–1700.11. Shingu Y, Komatsu S, Norimizu S, Taguchi Y, Sakamoto E. Laparoscopic subtotal cholecystectomy for severe cholecystitis. Surg Endosc. 2016; 30:526–531.12. Jain N, Neogi S, Bali RS, Harsh N. Relationship of gallbladder perforation and bacteriobilia with occurrence of surgical site infections following laparoscopic cholecystectomy. Minim Invasive Surg. 2015; 2015:204508.13. Park SJ, Lee KY, Park JW, Lee JG, Choi HJ, Chun HK, et al. A preliminary study for the development of indices and the current state of surgical site infections (SSIs) in Korea: the Korean Surgical Site Infection Surveillance (KOSSIS) program. Ann Surg Treat Res. 2015; 88:119–125.14. Kim J, Ihm C. Usefulness of bile cultures and predictive factors for bacteriobilia in percutaneous cholecystostomy in patients with acute cholecystitis. Korean J Lab Med. 2007; 27:281–285.15. Nakajima J, Sasaki A, Obuchi T, Baba S, Nitta H, Wakabayashi G. Laparoscopic subtotal cholecystectomy for severe cholecystitis. Surg Today. 2009; 39:870–875.16. Tian Y, Wu SD, Su Y, Kong J, Yu H, Fan Y. Laparoscopic subtotal cholecystectomy as an alternative procedure designed to prevent bile duct injury: experience of a hospital in northern China. Surg Today. 2009; 39:510–513.17. Jeong IO, Kim JY, Choe YM, Choi SK, Heo YS, Lee KY, et al. Efficacy and feasibility of laparoscopic subtotal cholecystectomy for acute cholecystitis. Korean J Hepatobiliary Pancreat Surg. 2011; 15:225–230.18. Cottier DJ, McKay C, Anderson JR. Subtotal cholecystectomy. Br J Surg. 1991; 78:1326–1328.19. Lee SI, Na BG, Yoo YS, Mun SP, Choi NK. Clinical outcome for laparoscopic cholecystectomy in extremely elderly patients. Ann Surg Treat Res. 2015; 88:145–151.20. Na BG, Yoo YS, Mun SP, Kim SH, Lee HY, Choi NK. The safety and efficacy of percutaneous transhepatic gallbladder drainage in elderly patients with acute cholecystitis before laparoscopic cholecystectomy. Ann Surg Treat Res. 2015; 89:68–73.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Laparoscopic Cholecystectomy and Minilaparotomy Cholecystectomy
- Laparoscopic Cholecystectomy in the Second Trimester of Pregnancy
- Korea University Experience in Laparoscopic Cholecystectomy
- A comparison od clinical results for laparoscopic cholecystectomy versus standard open cholecystectomy
- A Clinical Analysis of 300 Case of Laparoscopic Cholecystectomy
