Endovascular Treatment of Giant Serpentine Aneurysm of the Middle Cerebral Artery
- Affiliations
-
- 1Department of Neurosurgery, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea. jjongse@yonsei.ac.kr
- KMID: 2355652
- DOI: http://doi.org/10.7461/jcen.2016.18.3.264
Abstract
- Giant serpentine aneurysms are uncommon types of aneurysmal disease and have angiographically authentic features. We report a case of a 44-year-old male with headache and seizure. He presented a giant serpentine aneurysm arising from the middle cerebral artery (MCA). It was a large intracranial aneurysm thrombosed as a mass-like lesion while it maintained its outflow drainage into the distal MCA branches. The balloon occlusion test (BOT) was performed to test the tolerance of temporary collateral circulation. Following routine cerebral angiography, we performed an endovascular embolization on the proximal artery of MCA. He was discharged from the hospital with alert mental status and mild Gerstmann syndrome. The short-term follow-up imaging studies showed the decreased mass effect, and the patient presented an improved Gerstmann syndrome. After a careful evaluation of BOT, an endovascular embolization can be one of the powerful therapeutic instruments for giant serpentine aneurysm.
MeSH Terms
Figure
-
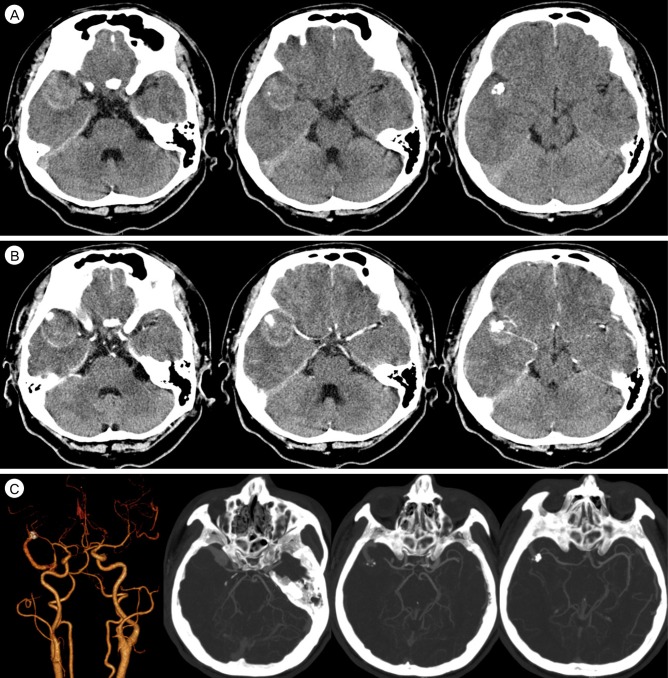
Fig. 1 Computed tomography (CT) images. (A) Pre-contrast CT shows scattered high density along the right bifurcation level of middle cerebral artery (MCA) and surrounding oval shaped, about 3.5 × 3.2 cm in size. (B) Post-contrast images shows heterogeneous high attenuation with tadpole like contrast enhancement along the right side Sylvian fissure. (C) CT angiography shows a feeding artery with a dilatation of right inferior division of MCA and an oval-shaped contrast pooling mass with considerable dilated outflow drainage and a mass effect.
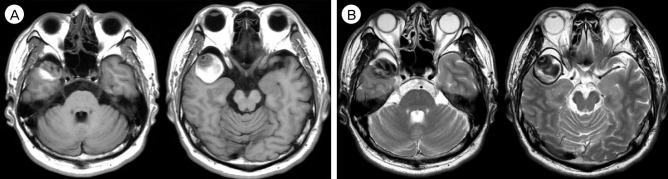
Fig. 2 Magnetic resonance imaging (MRI) images. (A) T1-weighted images (B) T2-weighted images. MRI shows a mass-like lesion with heterogenous signal intensity suggesting a formation of thrombus.
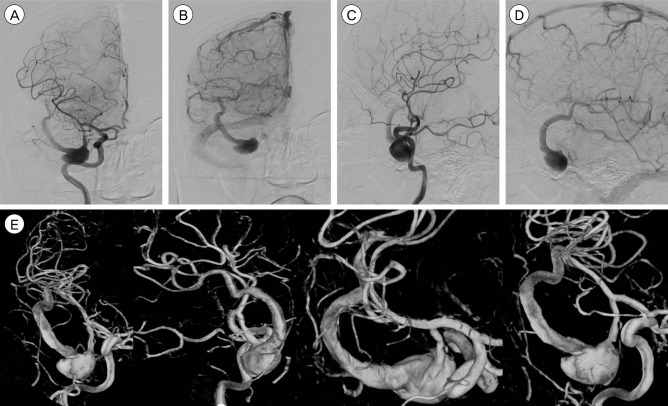
Fig. 3 Digital subtracted angiography (DSA) images. (A, B) Antero-posterior view (early, late), (C, D) Laterial views (early, late), (E) 3D-reconstructed images. DSA shows a giant aneurysm arising from the right middle cerebral artery (MCA) inferior trunk. The dilated outflow is seen as serpentine morphology which is continued to be drained to the distal MCA branches.
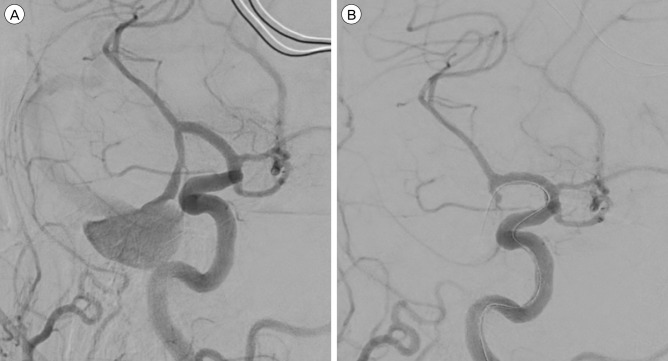
Fig. 4 BOT images. (A) Pre-test image, (B) Post-ballooning image. Balloon was located in the right MCA inferior trunk. After balloon inflation, an aneurysmal sac and its distal outflow was not seen. BOT = balloon occlusion test; MCA = middle cerebral artery.
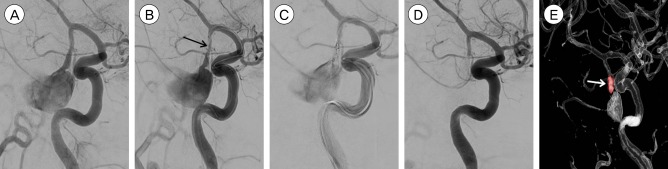
Fig. 5 Endovascular embolization. (A) Working view, (B) Double catheter technique. Catheter tip was placed in the proximal artery (black arrow), (C) Coil embolization, (D) Post-operative image, (E) Post-operative image of 3D reconstruction. Proximal artery was totally occluded by coiling (white arrow).
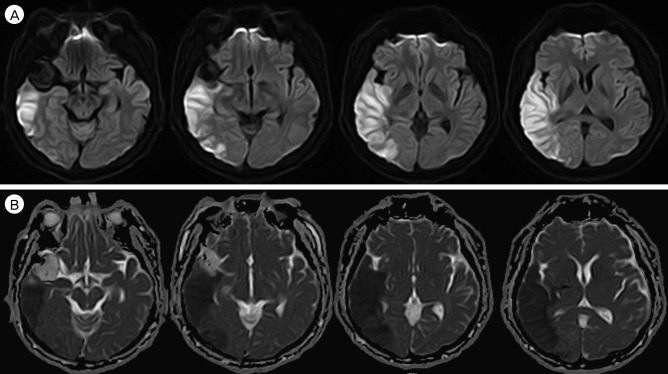
Fig. 6 Post-operative MRI images. (A) Diffusion-weighted images, (B) ADC images. A wedge-shaped focus of a tense and bright diffusion restriction involving both grey and white matter of right temporo-parietal lobe was observed. MRI = magnetic resonance image; ADC = apparent diffusion coefficients.
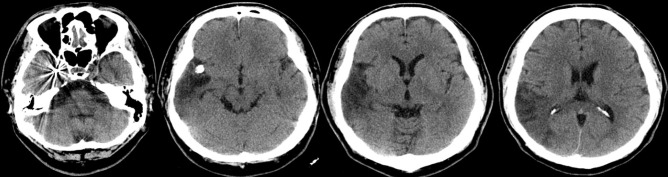
Fig. 7 Post-operative CT images. A metallic density was seen in the right temporal area as a coiling mass. Previous infarction area was decreased in the right temporo-parietal area. CT = computed tomography.
Reference
-
1. Aletich VA, Debrun GM, Monsein LH, Nauta HJ, Spetzler RF. Giant serpentine aneurysms: a review and presentation of five cases. AJNR Am J Neuroradiol. 1995; 5. 16(5):1061–1072. PMID: 7639128.2. Anson JA, Lawton MT, Spetzler RF. Characteristics and surgical treatment of dolichoectatic and fusiform aneurysms. J Neurosurg. 1996; 2. 84(2):185–193. PMID: 8592220.
Article3. Kumabe T, Kaneko U, Ishibashi T, Kaneko K, Uchigasaki S. Two cases of giant serpentine aneurysm. Neurosurgery. 1990; 6. 26(6):1027–1032. discussion 1032-3. PMID: 2362659.
Article4. Lee SJ, Ahn JS, Kwun BD, Kim CJ. Giant serpentine aneurysm of the middle cerebral artery. J Korean Neurosurg Soc. 2010; 8. 48(2):177–180. PMID: 20856671.
Article5. Mahadevan A, Tagore R, Siddappa NB, Santosh V, Yasha TC, Ranga U, et al. Giant serpentine aneurysm of vertebrobasilar artery mimicking dolichoectasia--an unusual complication of pediatric AIDS. Report of a case with review of the literature. Clin Neuropathol. 2008; Jan-Feb. 27(1):37–52. PMID: 18257473.6. Park JS, Lee MS, Kim MS, Kim DJ, Park JW, Whang K. Giant serpentine intracranial aneurysm: a case report. Korean J Radiol. 2001; Jul-Sep. 2(3):179–182. PMID: 11752991.
Article7. Sari A, Kandemir S, Kuzeyli K, Dinc H. Giant serpentine aneurysm with acute spontaneous complete thrombosis. AJNR Am J Neuroradiol. 2006; 4. 27(4):766–768. PMID: 16611761.8. Scott M, Skwarok E. The treatment of cerebral aneurysms by ligation of the common carotid artery. Surg Gynecol Obstet. 1961; 7. 113:54–61. PMID: 13749376.9. Segal HD, McLaurin RL. Giant serpentine aneurysm. Report of two cases. J Neurosurg. 1977; 1. 46(1):115–120. PMID: 830809.10. van Rooij WJ, Sluzewski M, Beute GN. Endovascular treatment of giant serpentine aneurysms. AJNR Am J Neuroradiol. 2008; 8. 29(7):1418–1419. PMID: 18388210.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Giant Serpentine Aneurysm of the Middle Cerebral Artery
- Giant Serpentine Intracranial Aneurysm Treated with Wrapping under the Extracorporeal Circulation and Hypothermia
- Giant Serpentine Aneurysm of the Posterior Cerebral Artery: Case Report
- Giant Serpentine Aneurysm of the Anterior Communicating Artery: Case Report
- Endovascular occlusion of giant serpentine aneurysm: A case report and literature review
