Radial Overgrowth after Surgical Treatment for Pediatric Distal Radius Fractures
- Affiliations
-
- 1Department of Orthopaedic Surgery, Kwangju Christian Hospital, Gwangju, Korea. stemcellchoi@hanmail.net
- KMID: 2355500
- DOI: http://doi.org/10.4055/jkoa.2016.51.5.365
Abstract
- PURPOSE
The purpose of this study was to examine the influence of radial overgrowth after surgical treatment for pediatric distal radius fractures.
MATERIALS AND METHODS
Twenty-two pediatric patients under the age of 10 years who underwent surgical treatment for a distal radius fracture without physeal injury were enrolled in this study. They were divided into 2 groups according to the ulnar fracture; distal radius alone fracture in 9 patients group and radioulnar both fracture in 13 patients group. The radial length, ulnar variance, and radial inclination at the last follow-up X-ray were measured using a simple lateral radiograph. The visual analogue scale (VAS) of distal radioulnar joint pain, the Mayo wrist score, and range of motion of the wrist were assessed for the clinical results.
RESULTS
At mean follow-up period of 3.7 years, radial overgrowth was 2.2 mm (p=0.01) compared with the un-injured side. There was negative ulnar variance on the injured side, an average of 0.8 mm (p=0.01). Clinically, mean VAS was 0.2, and the Mayo wrist score was 99.3. No significant difference in radial overgrowth (p=0.32), ulnar variance (p=0.99), VAS (p=0.29), and the Mayo wrist score (p=0.34) was observed between groups.
CONCLUSION
Radial overgrowth and negative ulnar variance was observed after surgical treatment of pediatric distal radius fracture without physeal injury. However, the radial overgrowth does not affect clinical outcomes.
Keyword
MeSH Terms
Figure
-

Figure 1 (A) Radial length was measured parallel to the long axis of the radius from radial head articular surface to distal radius articular surface in a simple forearm anteroposterior (AP) X-ray. In this patient, radial length discrepancy was 7.2 mm. (B) Ulnar variance was measured as the distance between a line perpendicular from the carpal joint surface of the distal end of the radius toward ulnar and the carpal surface of the ulnar in a simple forearm AP X-ray. Radial inclination was measured as the angle between one line connecting the radial styloid tip and ulnar aspect of the distal radius and a second line perpendicular to the longitudinal axis of the radius in a simple forearm AP X-ray. Radial inclination discrepancy was not seen in this patient.
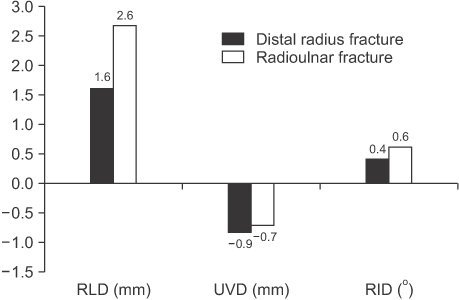
Figure 2 In radiologic results, there was no significant difference between distal radius fracture group and radioulnar fracture group. RLD, radial length discrepancy (p=0.32); UVD, ulnar variance discrepancy (p=0.99); RID, radial inclinatioin discrepancy (p=0.57).
Reference
-
1. Jones K, Weiner DS. The management of forearm fractures in children: a plea for conservatism. J Pediatr Orthop. 1999; 19:811–815.
Article2. Luhmann S, Gordon JE, Schoenecker PL. Intramedullary fixation of unstable both-bone forearm fractures in children. J Pediatr Orthop. 1998; 18:451–456.
Article3. Moon MS, Ok IY, Kim TH. Overgrowth after open reduction of femoral fracture in children. J Korean Orthop Assoc. 1990; 25:1391–1396.
Article4. Stephens MM, Hsu LC, Leong JC. Leg length discrepancy after femoral shaft fractures in children. Review after skeletal maturity. J Bone Joint Surg Br. 1989; 71:615–618.
Article5. Carsi B, Abril JC, Epeldegui T. Longitudinal growth after nonphyseal forearm fractures. J Pediatr Orthop. 2003; 23:203–207.
Article6. Yu Z, Wang Y, Wang C. The influence on radioulnar joints after single-bone fracture of the forearm in children. Zhonghua Wai Ke Za Zhi. 1996; 34:209–211.7. Crilly RG. Longitudinal overgrowth of chicken radius. J Anat. 1972; 112:11–18.8. Pablos J, Franzreb M, Barrios C. Longitudinal growth pattern of the radius after forearm fractures conservatively treated in children. J Pediatr Orthop. 1994; 14:492–495.9. Nielsen AB, Simonsen O. Displaced forearm fractures in children treated with AO plates. Injury. 1984; 15:393–396.
Article10. Zimmermann R, Gaschwentner M, Kralinger F, Arora R, Gabl M, Pechlaner S. Long-term results following pediatric distal forearm fractures. Arch Orthop Trauma Surg. 2004; 124:179–186.
Article11. Reynolds DA. Growth changes in fractured long-bones: a study of 126 children. J Bone Joint Surg Br. 1981; 63:83–88.
Article12. Griffin PP, Green WT. Fractures of the shaft of the femur in children: treatment and results. Orthop Clin North Am. 1972; 3:213–224.13. Shapiro F. Fractures of the femoral shaft in children. The overgrowth phenomenon. Acta Orthop Scand. 1981; 52:649–655.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Indications for Distal Radius Fractures
- Pediatric Fractures around the Wrist
- Surgical Treatment of the Distal Radius Fracture
- Surgical Treatment of Distal Radius Fractures and Treatment of Common Accompanying Lesions
- Treatment of Comminuted Distal Radius Fracutures with External Skeletal Fixation
