Intraoperative Monitoring and Mapping of the Functional Integrity of the Brainstem
- Affiliations
-
- 1Laboratory for Human and Experimental Neurophysiology, School of Medicine, Split, Croatia. vdeletis@chpnet.org
- 2Department of Intraoperative Neurophysiology, University Hospital of Bellvitge, Barcelona, Spain.
- KMID: 2354112
- DOI: http://doi.org/10.3988/jcn.2016.12.3.262
Abstract
- The risk of iatrogenic damage is very high in surgical interventions in or around the brainstem. However, surgical techniques and intraoperative neuromonitoring (ION) have evolved sufficiently to increase the likelihood of successful functional outcomes in many patients. We present a critical review of the methodologies available for intraoperative monitoring and mapping of the brainstem. There are three main groups of techniques that can be used to assess the functional integrity of the brainstem: 1) mapping, which provides rapid anatomical identification of neural structures using electrical stimulation with a hand-held probe, 2) monitoring, which provides real-time information about the functional integrity of the nervous tissue, and 3) techniques involving the examination of brainstem reflexes in the operating room, which allows for the evaluation of the reflex responses that are known to be crucial for most brainstem functions. These include the blink reflex, which is already in use, and other brainstem reflexes that are being explored, such as the masseter H-reflex. This is still under development but is likely to have important functional consequences. Today an abundant armory of ION methods is available for the monitoring and mapping of the functional integrity of the brainstem during surgery. ION methods are essential in surgery either in or around the brainstem; they facilitate the removal of lesions and contribute to notable improvements in the functional outcomes of patients.
Keyword
MeSH Terms
Figure
-
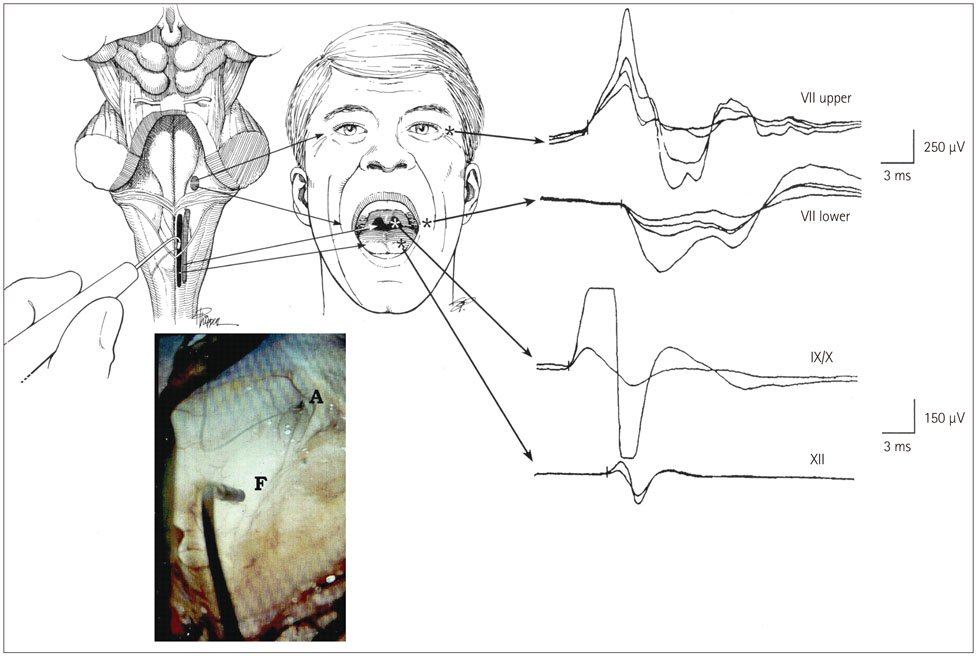
Fig. 1 Mapping of the brainstem cranial nerve motor nuclei (CMN). Upper left: drawing of the exposed floor of the fourth ventricle with the surgeon's hand-held stimulating probe in view. Upper middle: sites where hook-wire electrodes were inserted for recording muscle responses. Far upper right: compound muscle action potentials recorded from the orbicularis oculi and oris muscles after stimulation of the upper and lower facial nuclei (upper two traces), and from the pharyngeal wall and tongue muscles after stimulation of the CMN of cranial nerves IX, X, and XII (lower two traces). Lower left: photograph obtained with the aid of the operating microscope showing the hand-held stimulating probe placed on the floor of the fourth ventricle (F). A: aqueduct. Adapted from Morota et al., Neurosurgery 1995;37:922-929; discussion 929-930, with permission from Wolters Kluwer Health, Inc.10

Fig. 2 Typical patterns of CMN displacement by brainstem tumors in different locations. Upper and lower pontine tumors typically push the facial nuclei around the edge of the tumor, suggesting that it is necessary to precisely locate the facial nuclei before tumor resection in order to avoid them being damaged during surgery. Medullary tumors typically grow more exophytically and compress the lower CMN ventrally; these nuclei may be located on the ventral edge of the tumor cavity. Because of the interposed tumor, in these cases mapping before tumor resection usually does not allow identification of the CMN of cranial nerves IX, X, and XII. However, responses may be obtained close to the end of the tumor resection after most of the tumor tissue between the stimulating probe and the motor nuclei has been removed. Repeated mapping is recommended at this point since the risk of damaging motor nuclei is significantly higher than at the beginning of tumor debulking. Cervicomedullary junction spinal cord tumors simply push the lower CMN rostrally when they extend into the fourth ventricle. Adapted from Morota N, et al., Neurosurgery 1996;39:787-793; discussion 793-794, with permission from Wolters Kluwer Health, Inc.8 CMN: cranial nerve motor nuclei.
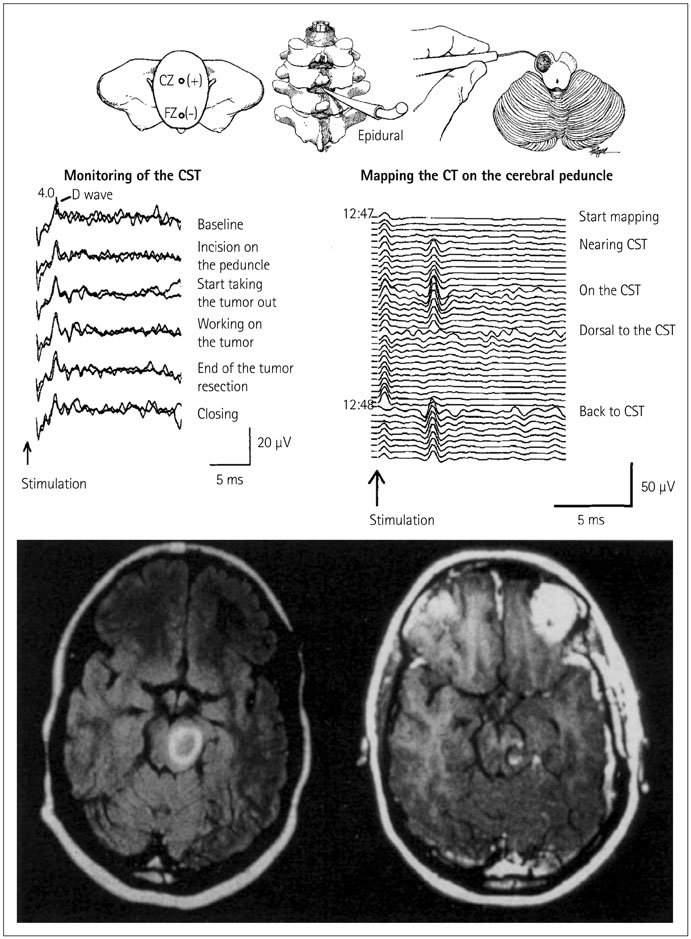
Fig. 3 Mapping and monitoring of the corticospinal tract (CST) during surgery for removing a left cerebral peduncle tumor in a 27-year-old woman. Bottom left: preoperative axial T1-weighted MR image with gadolinium enhancement revealed a high-intensity lesion in the left midbrain, dorsal to the cerebral peduncle. Bottom right: postoperative axial T1-weighted MR image with gadolinium enhancement showing that the tumor has been completely removed. The incision was performed in the area where no response to the stimulation of the cerebral peduncles was recorded. Top right: mapping of the CST on the cerebral peduncle is shown schematically. The cerebral peduncle is being mapped by a hand-held monopolar probe. As the probe neared the CST, responses were recorded from an epidural catheter (middle right). The responses were consistently reproducible. The stimulation intensity was 2 mA, the stimulation rate was 4 Hz, and four responses were averaged. Middle left: monitoring of the CST during tumor resection. After CST mapping, motor evoked potentials were continuously monitored by recording D-waves epidurally after transcranial electrical stimulation. The D-waves remained stable throughout the procedure and, the patient's preoperative motor function reappeared postoperatively. Adapted from Deletis V, et al., Operative Tech Neurosurg 2000;2:109-113, with permission from Elsevier.14
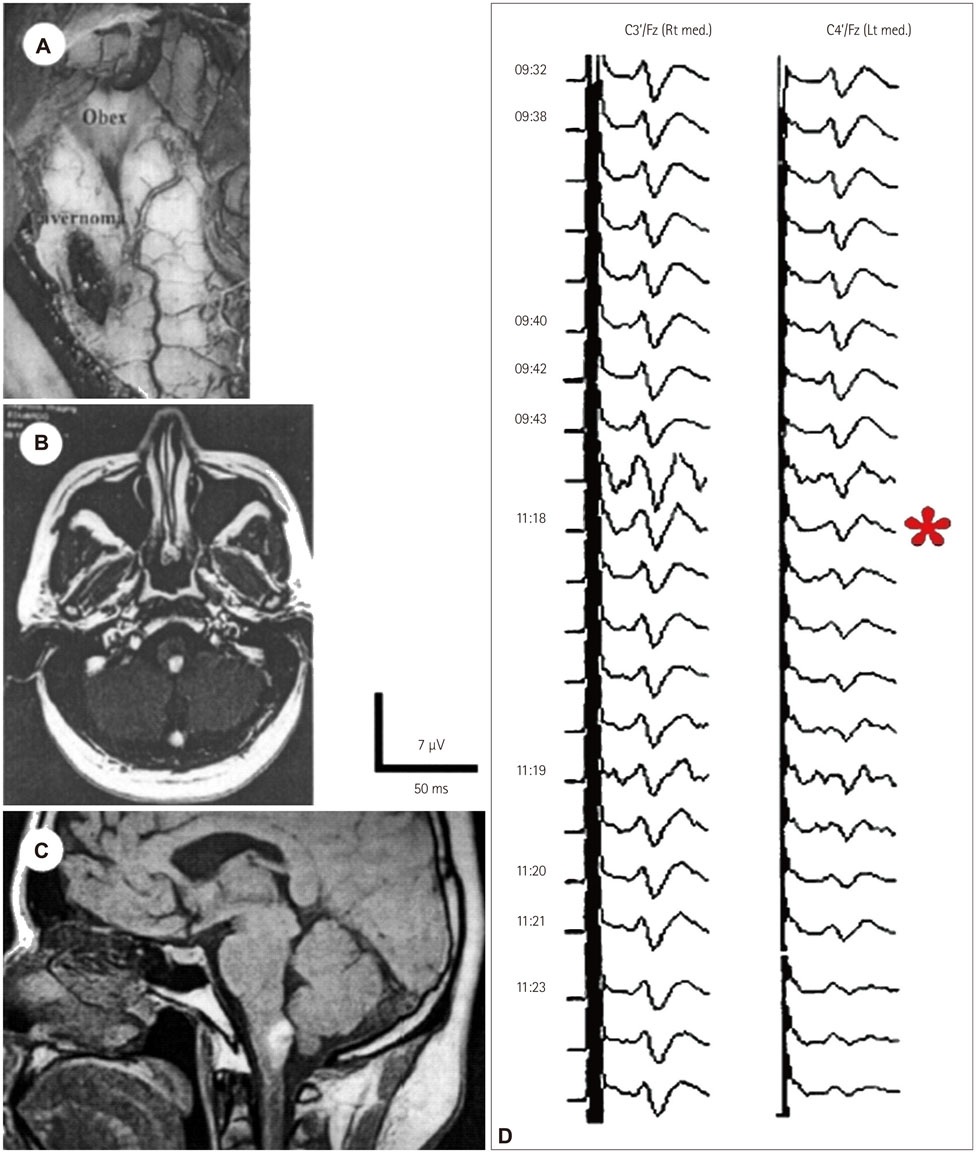
Fig. 4 Intraoperative microscope photograph (A) illustrating the location of the cavernoma in the left hemimedulla. Preoperative axial (B) and sagittal (C) T1-weighted MR images showed a hyperintense lesion in the left dorsal medulla in a 26-year-old patient. Monitoring (D) of the somatosensory-evoked potentials (SEPs) during surgical removal of the cavernoma disclosed a selective lesion in the left dorsal column nuclei. During the initial incision in the region of the dorsal column nuclei, SEPs after the left median nerve stimulation diminished (*) and subsequently disappeared (not shown), whereas SEPs from the right median nerve remained intact. The patient woke up after surgery with significant sensory loss in the left arm. In this patient we could only document the lesion, being unable to remove it. Adapted from Deletis V, et al., Operative Tech Neurosurg 2000;2:109-113, with permission from Elsevier.14

Fig. 5 Intraoperative schematic of eliciting and recording of corticobulbar motor-evoked potentials (CoMEPs). Lower left: schematic of positioning the stimulating electrode over the scalp. Upper left: schematic of the corticobulbar pathways innervating CMN (cranial nerves VII, IX, X, and XII). Middle: positioning the recording electrodes inserted in the orbicularis oris, pharyngeal, tongue, and vocal muscles (cranial nerves VII, IX, XII, and X, respectively) to monitor CoMEPs. To the right: typical examples of CoMEPs recorded from muscles innervated by cranial motor nerves.
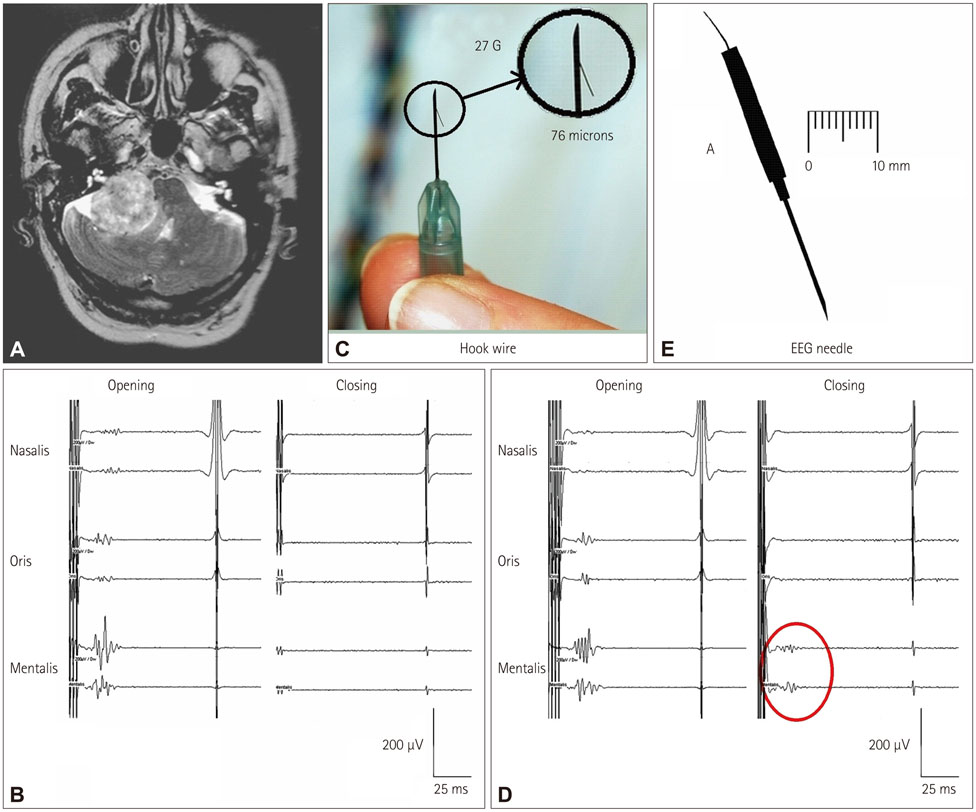
Fig. 6 CoMEPs recorded from the mentalis muscle after TES of the motor cortex in a patient with a vestibular schwannoma. A: Axial MR image showing a right vestibular schwannoma. B: Facial CoMEPs recorded with hook-wire electrodes (C) from the mentalis muscle. The facial nerve was accidentally damaged during surgery, after which the facial CoMEPs disappeared (closing). D: Facial CoMEPs recorded with an EEG needle (E) from the mentalis muscle. After damaging the facial nerve there was still a recordable response (red circle), which was considered to be a far-field response of surrounding muscles such as those of the tongue (closing). Adapted from Fernandez-Conejero I, et al., J Neurosurg 2014;120:291-292, with permission from American Association of Neurological Surgeons.21 CoMEPs: corticobulbar motor-evoked potentials.
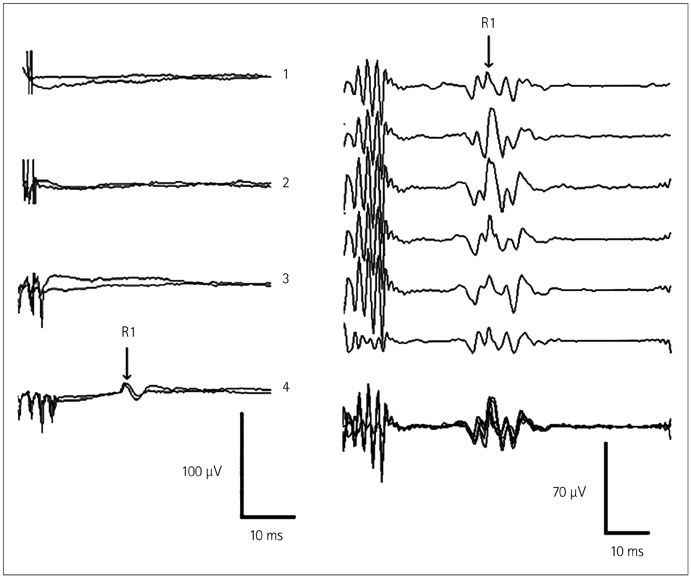
Fig. 7 Recording the R1 component of the blink reflex (BR). To the left: recordings of the R1 component of the BR from one patient. In this patient a train of four stimuli elicited the responses, whereas trains consisting of one, two, or three stimuli did not. Each trace represents the average of two responses. To the right: recordings of the R1 component of the BR from another patient showing the high reproducibility of the responses. Each trace represents the average of two responses. The last trace represents the superposition of the first six. Adapted from Deletis V, et al., Muscle Nerve 2009;39:642-646, with permission from Wiley Periodicals, Inc.25
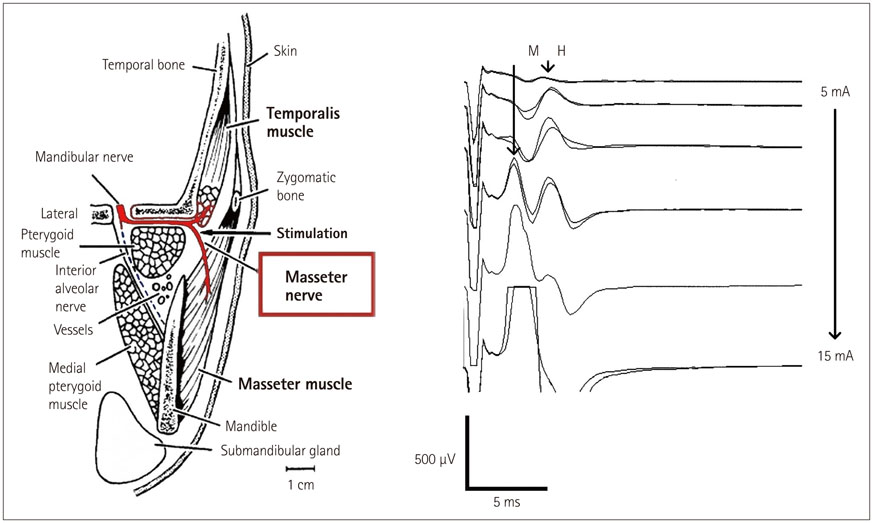
Fig. 8 Recording M-responses and H-reflexes from the masseter muscle. To the left: schematic of the anatomy of the masseter nerve innervating the masseter and temporalis muscles. To the right: after stimulation, masseter nerve recordings of the H-reflexes and M-responses of the masseter muscle were found to be correlated with the stimulus intensities. Adapted from Godaux E, et al., Brain Res 1975;85:447-458, with with permission from Elsevier26 (to the left) and Téllez et al. 2015 (personal communications) (to the right).
Reference
-
1. Neuloh G, Bogucki J, Schramm J. Intraoperative preservation of corticospinal function in the brainstem. J Neurol Neurosurg Psychiatry. 2009; 80:417–422.
Article2. Dong CC, Macdonald DB, Akagami R, Westerberg B, Alkhani A, Kanaan I, et al. Intraoperative facial motor evoked potential monitoring with transcranial electrical stimulation during skull base surgery. Clin Neurophysiol. 2005; 116:588–596.
Article3. Deletis V, Fernandez-Conejero I, Ulkatan S, Costantino P. Methodology for intraoperatively eliciting motor evoked potentials in the vocal muscles by electrical stimulation of the corticobulbar tract. Clin Neurophysiol. 2009; 120:336–341.
Article4. Deletis V, Fernández-Conejero I, Ulkatan S, Rogić M, Carbó EL, Hiltzik D. Methodology for intra-operative recording of the corticobulbar motor evoked potentials from cricothyroid muscles. Clin Neurophysiol. 2011; 122:1883–1889.
Article5. Strauss C, Romstöck J, Nimsky C, Fahlbusch R. Intraoperative identification of motor areas of the rhomboid fossa using direct stimulation. J Neurosurg. 1993; 79:393–399.
Article6. Morota N, Deletis V. The importance of brainstem mapping in brainstem surgical anatomy before the fourth ventricle and implication for intraoperative neurophysiological mapping. Acta Neurochir (Wien). 2006; 148:499–509. discussion 509.
Article7. Deletis V. Evoked Potentials. In : Lake CL, editor. Clinical Monitoring for Anesthesia and Critical Care. 2nd ed. Lake Carol: W.B. Saunders;1994. p. 282–314.8. Morota N, Deletis V, Lee M, Epstein FJ. Functional anatomic relationship between brain-stem tumors and cranial motor nuclei. Neurosurgery. 1996; 39:787–793. discussion 793-794.
Article9. Liscić RM, Morota N, Deletis V. Intramedullar stimulation of the facial and hypoglossal nerves: estimation of the stimulated site. Croat Med J. 2000; 41:384–388.10. Morota N, Deletis V, Epstein FJ, Kofler M, Abbott R, Lee M, et al. Brain stem mapping: neurophysiological localization of motor nuclei on the floor of the fourth ventricle. Neurosurgery. 1995; 37:922–929. discussion 929-930.11. Romstöck J, Strauss C, Fahlbusch R. Identification of cranial nerve nuclei. Muscle Nerve. 2000; 23:1445–1446.
Article12. Romstöck J, Strauss C, Fahlbusch R. Continuous electromyography monitoring of motor cranial nerves during cerebellopontine angle surgery. J Neurosurg. 2000; 93:586–593.
Article13. Prell J, Strauss C, Rachinger J, Scheller C, Alfieri A, Herfurth K, et al. The intermedius nerve as a confounding variable for monitoring of the free-running electromyogram. Clin Neurophysiol. 2015; 126:1833–1839.
Article14. Deletis V, Sala F, Morota N. Intraoperative neurophysiological monitoring and mapping during brain stem surgery: a modern approach. Oper Tech Neurosurg. 2000; 2:109–113.
Article15. Fahlbusch R, Strauss C. [Surgical significance of cavernous hemangioma of the brain stem]. Zentralbl Neurochir. 1991; 52:25–32.16. Polo G, Fischer C, Sindou MP, Marneffe V. Brainstem auditory evoked potential monitoring during microvascular decompression for hemifacial spasm: intraoperative brainstem auditory evoked potential changes and warning values to prevent hearing loss--prospective study in a consecutive series of 84 patients. Neurosurgery. 2004; 54:97–104. discussion 104-106.
Article17. Quiñones-Hinojosa A, Alam M, Lyon R, Yingling CD, Lawton MT. Transcranial motor evoked potentials during basilar artery aneurysm surgery: technique application for 30 consecutive patients. Neurosurgery. 2004; 54:916–924. discussion 924.
Article18. Macdonald DB, Skinner S, Shils J, Yingling C. American Society of Neurophysiological Monitoring. Intraoperative motor evoked potential monitoring - a position statement by the American Society of Neurophysiological Monitoring. Clin Neurophysiol. 2013; 124:2291–2316.
Article19. Verst SM, Sucena AC, Maldaun MV, Aguiar PH. Effectiveness of C5 or C6-Cz assembly in predicting immediate post operative facial nerve deficit. Acta Neurochir (Wien). 2013; 155:1863–1869.
Article20. Ulkatan S, Deletis V, Fernandez-Conejero I. Central or peripheral activations of the facial nerve? J Neurosurg. 2007; 106:519–520. author reply 520.
Article21. Fernández-Conejero I, Deletis V. Transcranial electrical stimulation and monitoring. J Neurosurg. 2014; 120:291–292.22. Bostock H, Lin CS, Howells J, Trevillion L, Jankelowitz S, Burke D. After-effects of near-threshold stimulation in single human motor axons. J Physiol. 2005; 564(Pt 3):931–940.
Article23. Fernández-Conejero I, Ulkatan S, Sen C, Deletis V. Intra-operative neurophysiology during microvascular decompression for hemifacial spasm. Clin Neurophysiol. 2012; 123:78–83.
Article24. Malcharek MJ, Landgraf J, Hennig G, Sorge O, Aschermann J, Sablotzki A. Recordings of long-latency trigeminal somatosensoryevoked potentials in patients under general anaesthesia. Clin Neurophysiol. 2011; 122:1048–1054.
Article25. Deletis V, Urriza J, Ulkatan S, Fernandez-Conejero I, Lesser J, Misita D. The feasibility of recording blink reflexes under general anesthesia. Muscle Nerve. 2009; 39:642–646.
Article26. Godaux E, Desmedt JE. Exteroceptive suppression and motor control of the masseter and temporalis muscles in normal man. Brain Res. 1975; 85:447–458.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Advancing Intraoperative Neurophysiological Monitoring With Human Reflexes
- Interruption of bispectral index monitoring by nerve integrity monitoring during tympanoplasty: A case report
- The Comparison of the Anesthetic Regimens for Functional Direct Cortical Stimulation Mapping during Craniotomy
- Microvascular Decompression for Tinnitus
- Surgery for seizure-related structural lesions of the brain with intraoperative acute recording(ECoG) and functional mapping
