Concurrent Mucosal Melanoma and Angiofibroma of the Nose
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, The Catholic University of Korea College of Medicine, Seoul, Korea. fpsljh@gmail.com
- 2Department of Pathology, The Catholic University of Korea College of Medicine, Seoul, Korea.
- KMID: 2353628
- DOI: http://doi.org/10.21053/ceo.2015.01333
Abstract
- Malignant melanoma rarely develops in the paranasal sinuses, and generally has a poor prognosis. However, mucosal melanoma can masquerade both clinically and histopathologically as a benign lesion, rendering accurate early diagnosis difficult. On the other hand, angiofibroma, a benign tumor, is more easily diagnosed than a mucosal melanoma, because the former exhibits specific histopathological features. No cases of concurrent angiofibroma and mucosal melanoma have been reported to date. We describe such a case below.
Keyword
Figure
-
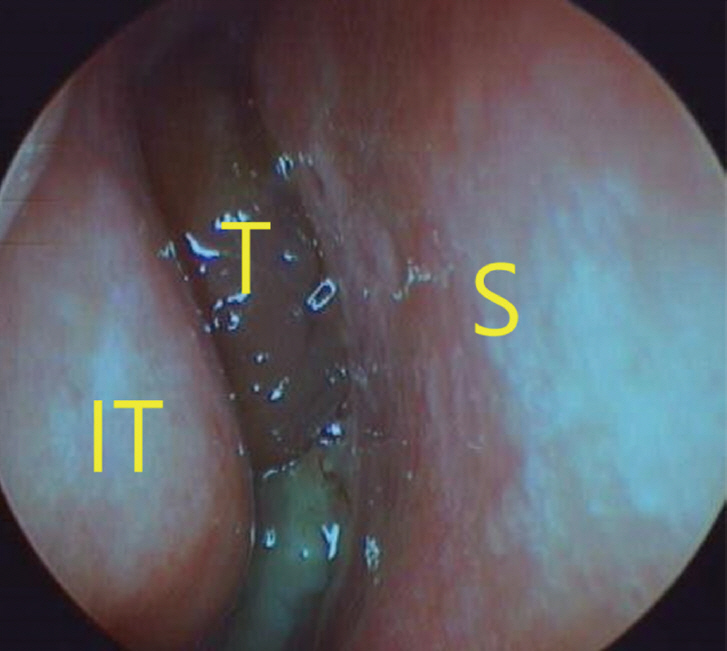
Fig. 1. Preoperative endoscopic fi ndings in the right nasal cavity. S, septum; IT, inferior turbinate; T, tumor.
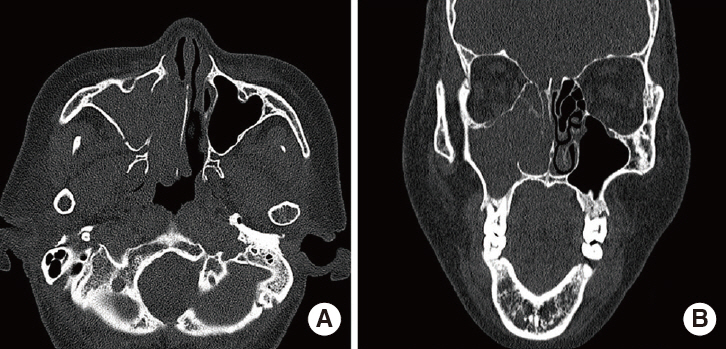
Fig. 2. Computed tomography reveals dense soft tissue in the right maxillary sinus and right nasal cavity. (A) Axial, (B) coronal images.

Fig. 3. Paranasal sinus magnetic resonance imaging fi ndings. An enhanced right antral mass with a widened maxillary ostium is evident; it extends into the right nasal cavity axial T2-weighted (A), axial T1-weighted (B), and coronal gadolinium-enhanced T1-weighted (C) images.

Fig. 4. Angiography with tumor embolization. The tumor was supplied by nasal branch of right sphenopalatine artery. (A) Before embolization, (B) after embolization.

Fig. 5. (A) Mucosal melanoma with an angiofi broma. Mucosal hyperpigmentation in subepithelium showing admixture of thin walled blood vessels and fi brous stroma (H&E: a, ×40; b, ×100). (B) The angiofi broma lesion of the specimen. Nasal mucosa with fi broblastic stroma and thin walled blood vessels (H&E, ×40). (C) Mucosal melanoma with intracytoplasmic melanic pigment (H&E: a, ×100; b, ×400). (D) Tumor cells positive for Melan-A (×40).
Reference
-
1. Medhi P, Biswas M, Das D, Amed S. Cytodiagnosis of mucosal malignant melanoma of nasal cavity: A case report with review of literature. J Cytol. 2012; Jul. 29(3):208–10.
Article2. Mihajlovic M, Vlajkovic S, Jovanovic P, Stefanovic V. Primary mucosal melanomas: a comprehensive review. Int J Clin Exp Pathol. 2012; Oct. 5(8):739–53.3. Mundra RK, Sikdar A. Endoscopic removal of malignant melanoma of the nasal cavity. Indian J Otolaryngol Head Neck Surg. 2005; Oct. 57(4):341–3.
Article4. Rinaldo A, Shaha AR, Patel SG, Ferlito A. Primary mucosal melanoma of the nasal cavity and paranasal sinuses. Acta Otolaryngol. 2001; Dec. 121(8):979–82.
Article5. Mendenhall WM, Amdur RJ, Hinerman RW, Werning JW, Villaret DB, Mendenhall NP. Head and neck mucosal melanoma. Am J Clin Oncol. 2005; Dec. 28(6):626–30.
Article6. Grant-Kels JM, Bason ET, Grin CM. The misdiagnosis of malignant melanoma. J Am Acad Dermatol. 1999; Apr. 40(4):539–48.
Article7. Clifton N, Harrison L, Bradley PJ, Jones NS. Malignant melanoma of nasal cavity and paranasal sinuses: report of 24 patients and literature review. J Laryngol Otol. 2011; May. 125(5):479–85.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Labial Mucosal Melanoma Metastasized to the Lung
- Facial Translocation Approach for Nasopharyngeal Angiofibroma
- Four Cases of Primary Malignant Melanoma of the Nasal Cavity
- Mucosal Malignant Melanomas of the Nasal Cavity and Paranasal Sinuses: Clinical Characteristics and Treatment Outcomes
- Primary Angiofibroma Developed in the Orbit
