Adult-Onset Asthma and Periocular Xanthogranuloma in a 75-Year-Old Man
- Affiliations
-
- 1Department of Ophthalmology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. ydkimoph@skku.edu
- 2Department of Ophthalmology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- KMID: 2351879
- DOI: http://doi.org/10.3341/jkos.2016.57.9.1465
Abstract
- PURPOSE
Adult xanthogranulomatous disease of the orbit including adult-onset asthma and periocular xanthogranuloma is rare. To the best of the author's knowledge, adult-onset asthma and periocular xanthogranuloma have not been previously reported in Korea.
CASE SUMMARY
A 75-year-old man presented with a 15-year history of progressive bilateral yellowish eyelid mass. He had a history of adult-onset asthma diagnosed 13 years ago. On ocular examination, there were firm yellowish bilateral eyelid masses and ptosis markedly on the right eye. Exophthalmos was noted in the right eye. There were exotropia, hypertropia, and gaze restriction of the right eye. Orbit magnetic resonance imaging demonstrated an ill-defined bilateral infiltrative orbital mass extending to the lid, lacrimal gland, and sinuses. A right orbital mass extended to the posterior orbit. Enlargement of extraocular muscles was also noted in the right eye. Left upper eyelid mass debulking surgery was performed. A combination therapy of azathioprine and prednisolone was started. Mass debulking surgeries of the right upper and lower eyelids were performed.
CONCLUSIONS
Adult-onset asthma and periocular xanthogranuloma is known as a refractory disease. Combination therapy with azathioprine and steroid therapy with mass debulking surgery is a good treatment option for adult-onset asthma and periocular xanthogranuloma.
Keyword
MeSH Terms
Figure
-
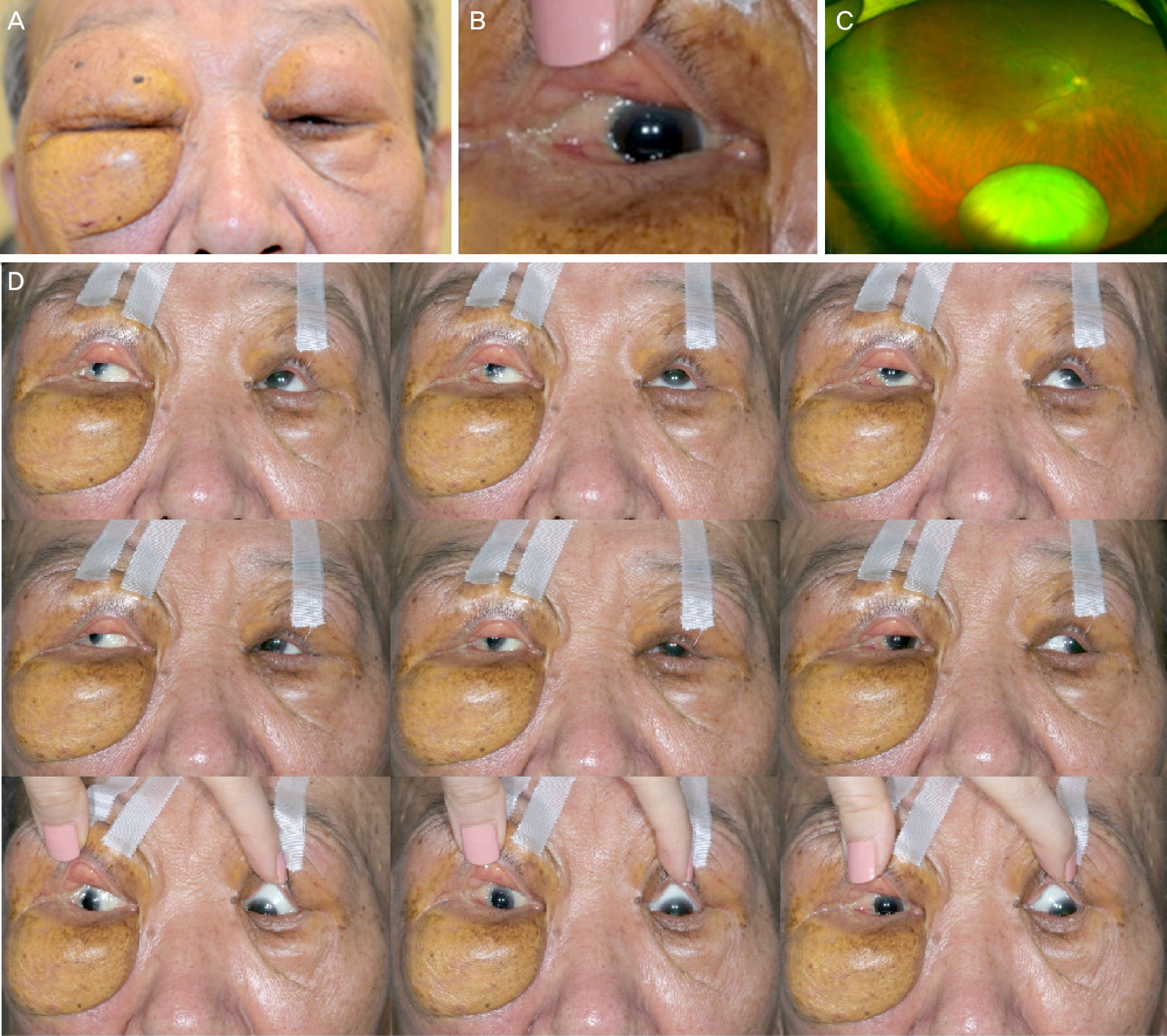
Figure 1. Clinical photographs of patient. (A) Clinical photograph of patient shows bilateral eyelid mass with yellowish pigmentation and severe ptosis more marked in the right eye. (B) Yellowish infiltration of the right temporal and inferior bulbar conjunctiva is noted. (C) Ultra-widefield retinal imaging reveals crystalline lens dislocation into the vitreous cavity of right eye. (D) There are exotropia and hypertropia of right eye on primary gaze and restriction of upward, downward, and medial gaze.

Figure 2. Orbit magnetic resonance imaging taken 2 years ago demonstrates ill-defined bilateral infiltrative orbital mass extending to lid, lacrimal gland, anterior orbit, nasal cavity, and sinuses. Mass infiltrates posterior orbit and extraocular muscles of right eye. Mass shows low signal intensity on T1-weighted images (T1WI) (A, B), heterogeneous high signal intensity on T2-weighted images (T2WI) (C, D), and strong enhancement by gadolinium contrast medium (T1 c CE) (E, F). Crystalline lens is not dislocated. After 2 years, orbital mass enlarges and infiltrates entire orbit (G-L). Exophthalmos progressed. Right orbital mass extends to orbital apex and enlargement of extraocular muscles is aggravated. Crystalline lens is dislocated into the vitreous cavity.
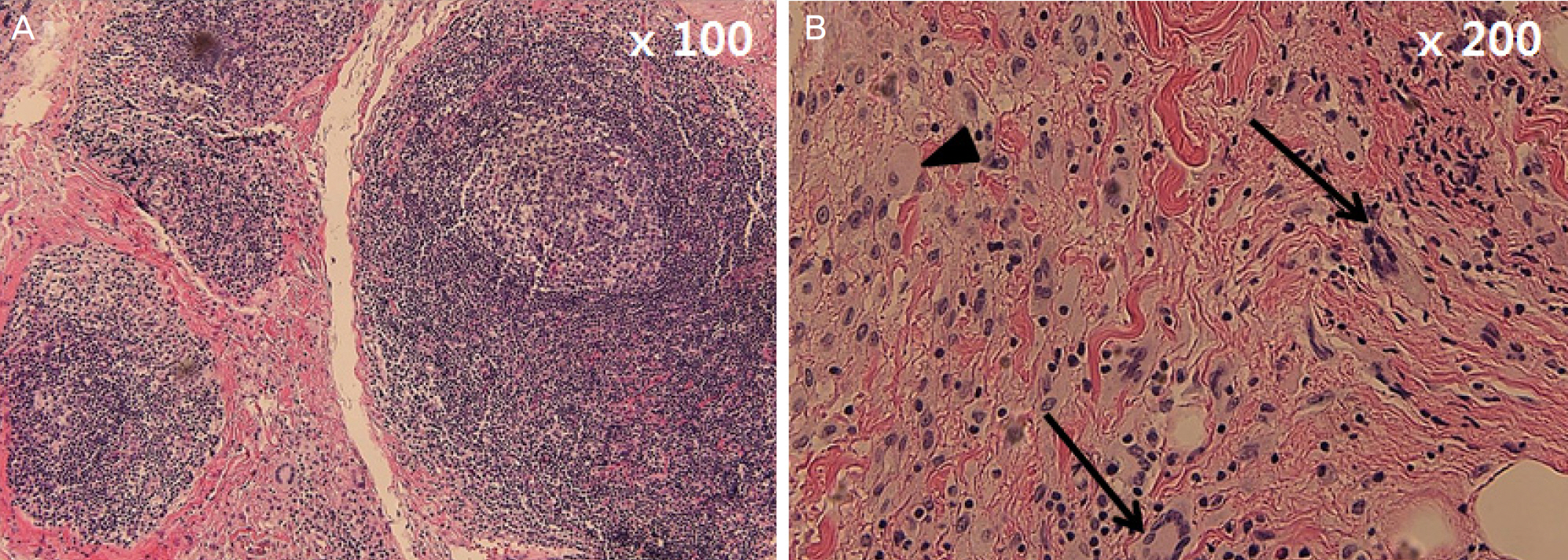
Figure 3. Histopathological examination of mass. (A) Histopathology shows granulomatous infiltration consisted of Touton giant cells, xanthoma cells (foamy histiocytes), and inflammatory cells with follicle formation (hematoxylin-eosin, ×100). (B) The section demonstrates Touton giant cells (arrows) and xanthoma cells (arrowhead) (hematoxylin-eosin, ×200).
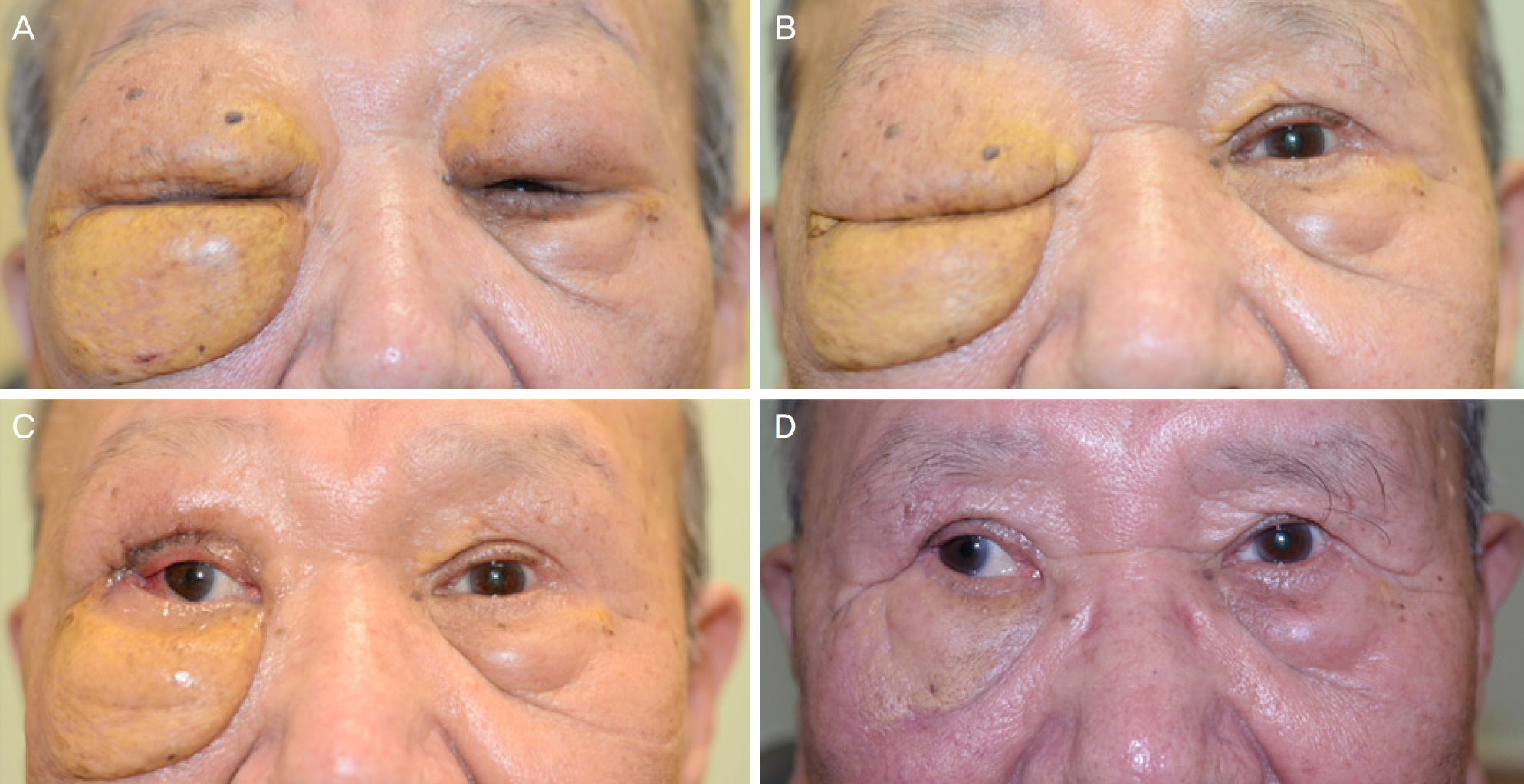
Figure 4. Serial preoperative and postoperative photographs of patient. (A) Clinical photograph of the patient before treatment shows bilateral eyelid mass and severe ptosis more marked in the right eye. (B) Left eyelid ptosis is improved two months after levator resection and mass debulking surgery of left upper eyelid. Note decreased tumor infiltration of right eyelid after systemic use of steroid and azathioprine. (C) One month after right upper eyelid surgery, improvement of right eyelid ptosis is noted. (D) Right lower eyelid mass is also improved one year after right lower eyelid surgery. There is marked improvement of eyelid mass with sat-isfactory cosmetic result.
Reference
-
References
1. Bijlsma WR, van den Bosch WA, van Daele PL, Paridaens D. Azathioprine and prednisone combination treatment for adult periocular and orbital xanthogranulomatous disease. Acta Ophthalmol. 2011; 89:e278–82.
Article2. Jakobiec FA, Mills MD, Hidayat AA, et al. Periocular xanthogra-nulomas associated with severe adult-onset asthma. Trans Am Ophthalmol Soc. 1993; 91:99–125. discussion 125–9.3. Guo J, Wang J. Adult orbital xanthogranulomatous disease: review of the literature. Arch Pathol Lab Med. 2009; 133:1994–7.
Article4. Alper MG, Zimmerman LE, Piana FG. Orbital manifestations of Erdheim-Chester disease. Trans Am Ophthalmol Soc. 1983; 81:64–85.5. Robertson DM, Winkelmann RK. Ophthalmic features of necrobiotic xanthogranuloma with paraproteinemia. Am J Ophthalmol. 1984; 97:173–83.
Article6. Sivak-Callcott JA, Rootman J, Rasmussen SL, et al. Adult xanthogranulomatous disease of the orbit and ocular adnexa: new immunohistochemical findings and clinical review. Br J Ophthalmol. 2006; 90:602–8.
Article7. Hammond MD, Niemi EW, Ward TP, Eiseman AS. Adult orbital xanthogranuloma with associated adult-onset asthma. Ophthal Plast Reconstr Surg. 2004; 20:329–32.
Article8. Murray D, Marshall M, England E, et al. Erdheim-Chester disease. Clin Radiol. 2001; 56:481–4.
Article9. Elner VM, Mintz R, Demirci H, Hassan AS. Local corticosteroid treatment of eyelid and orbital xanthogranuloma. Trans Am Ophthalmol Soc. 2005; 103:69–73. discussion 73–4.
Article10. Shams PN, Rasmussen SL, Dolman PJ. Adult-onset asthma abdominal with simultaneous conjunctival, eyelid, and orbital xanthog-ranulomatosis responsive to systemic immunosuppression. Ophthal Plast Reconstr Surg. 2015; 31:e162–3.11. Papagoras C, Kitsos G, Voulgari PV, et al. Periocular xanthogranuloma: a forgotten entity? Clin Ophthalmol. 2010; 4:105–10.12. Hayden A, Wilson DJ, Rosenbaum JT. Management of orbital xanthogranuloma with methotrexate. Br J Ophthalmol. 2007; 91:434–6.
Article13. Ho VH, Chevez-Barrios P, Jorgensen JL, et al. Receptor expression in orbital inflammatory syndromes and implications for targeted therapy. Tissue Antigens. 2007; 70:105–9.
Article14. Chung SJ, Lew H. Adult orbital xanthogranulomatous disease in a 42-year-old woman. J Korean Ophthalmol Soc. 2011; 52:975–8.
Article15. Choi HJ, Kwon HJ, Kim HY. A case of posttraumatic necrobiotic xanthogranuloma of the orbit. J Korean Ophthalmol Soc. 2008; 49:677–80.
Article
