Iris-trabecular Contact Index Change after Cataract Surgery in Acute Angle Closure Glaucoma
- Affiliations
-
- 1Busan Sungmo Eye Hospital, Busan, Korea. sungmobusan@hanmail.net
- KMID: 2351870
- DOI: http://doi.org/10.3341/jkos.2016.57.9.1400
Abstract
- PURPOSE
To evaluate the change of iris-trabecular contact index (ITC index) after cataract surgery in acute angle closure glaucoma.
METHODS
Twelve patients (17 eyes) who had a history of acute angle closure glaucoma underwent swept source optical coherence tomography before and after cataract surgery. Correlations between lens vault (LV), ITC index and intraocular pressure (IOP), anterior chamber depth (ACD), anterior chamber volume (ACV), and angle parameters were analyzed before and after cataract surgery.
RESULTS
IOP (p = 0.007), ACD (p < 0.001), ACV (p < 0.001), angle parameters (p = 0.001), and ITC index (p = 0.012) were improved after cataract surgery. ITC index decreased from 88.42 ± 23.59% to 48.91 ± 35.13% after cataract surgery (p = 0.012). There was no correlation between LV and ACD (p = 0.075), ACV (p = 0.864), angle parameter (p = 0.112-0.707), or ITC index (p = 0.288) before cataract surgery. The correlations between ITC index and IOP (p = 0.021), ACD (p = 0.002), ACV (p < 0.001), and angle parameter (p = 0.001-0.030) were statistically significant before surgery but not statistically significant (p = 0.223/0.206/0.761/ 0.096-0.819) after surgery.
CONCLUSIONS
ITC index significantly improved after cataract surgery, but part of angle closure was not resolved in some cases of acute angle closure glaucoma.
MeSH Terms
Figure
-
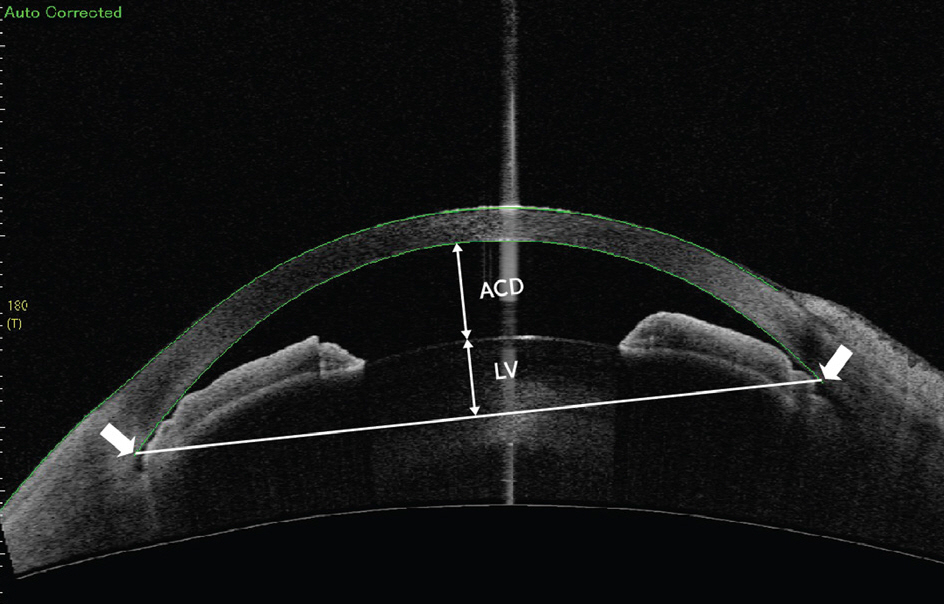
Figure 1. Swept source optical coherence tomography image illustrating anterior chamber depth (ACD) and lens vault (LV). White arrows indicate the scleral spur.
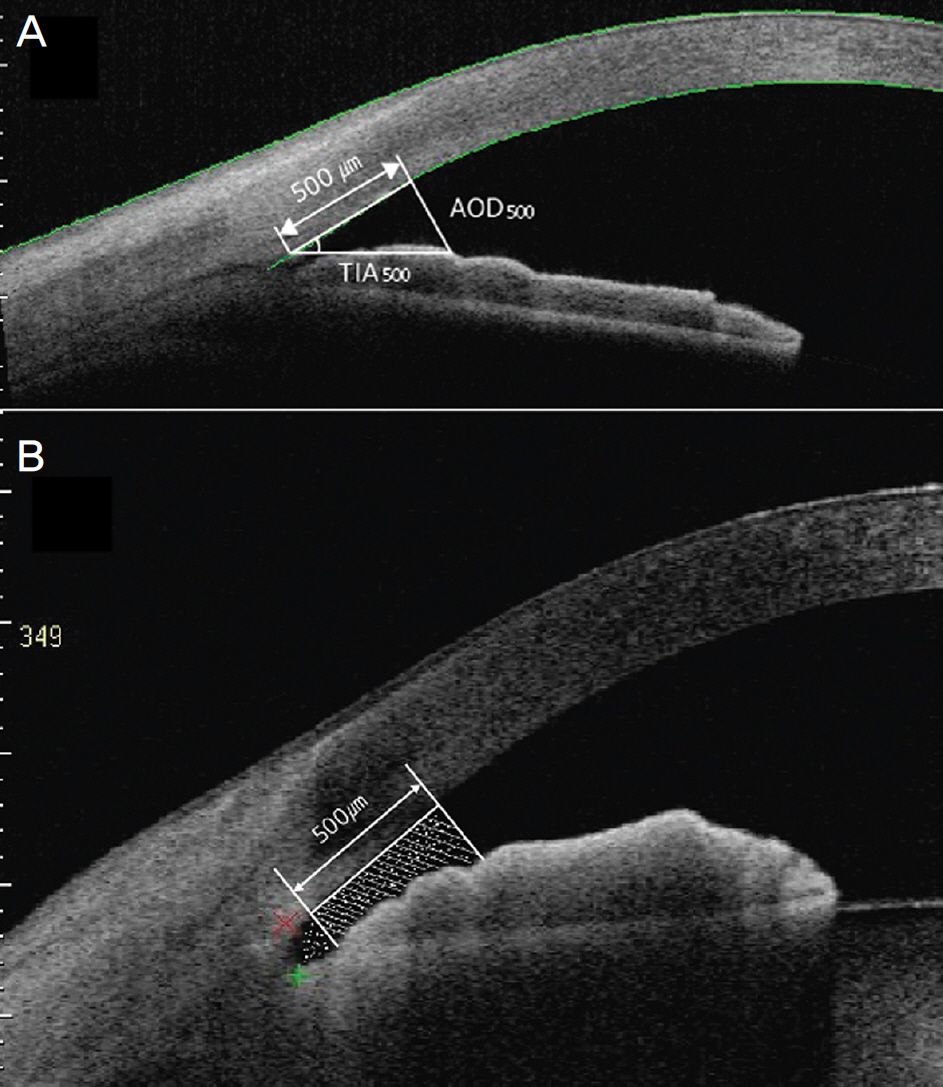
Figure 2. Cross-section image of angle structure illustrating angle parameters. (A) Angle opening distance at 500 μ m from scleral spur (AOD500) and trabecular-iris angle 500 (TIA500). (B) Trabecular-iris surface area 500 (TISA500) is expressed by dot printed and angle recess area 500 (ARA500) is expressed by a hatched box.
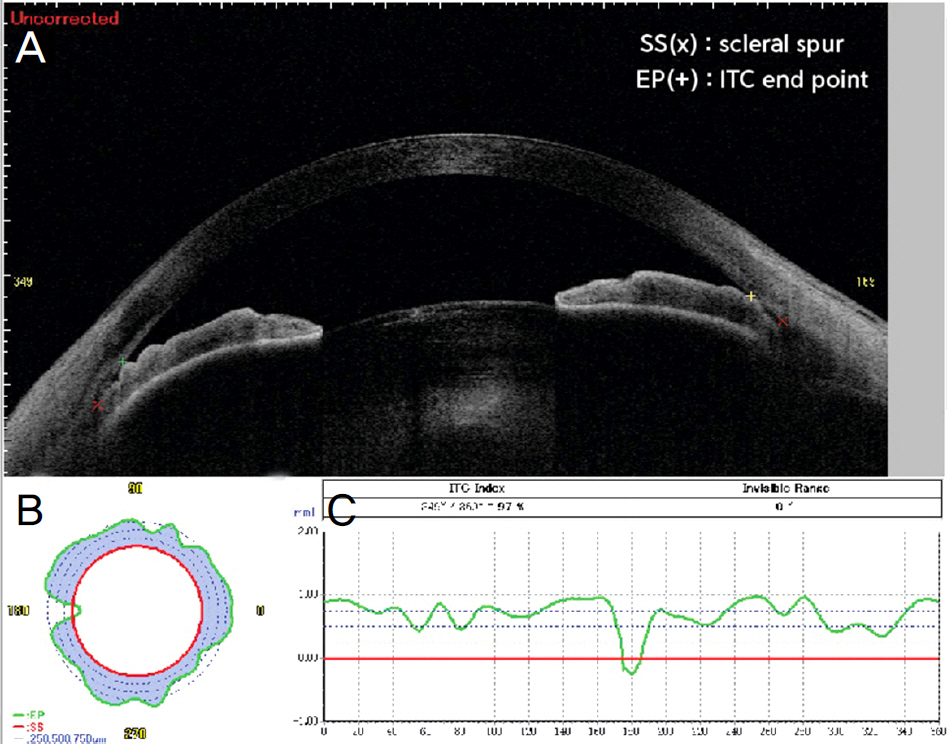
Figure 3. Swept source optical coherence tomography image illustrating a single frame of anterior chamber. (A) The red colored “x” are the scleral spurs (SS) and the “+” are the iris-trabecular contact end points (EP). (B) Iris-trabecular con-tract (ITC) chart with blue area representing the amount and the distribution of iris-trabecular contact. Red line is the consecutive line of the scleral spur and the green line is the consecutive line of end point. (C) Iris-trabecular contact graph with X axis representing the degree of the angle, Y axis repre-senting iris-trabecular contact. “+” means the contact with iris and trabecular meshwork and “-” means non-contact between the two structures.
Reference
-
References
1. Lowe RF. Aetiology of the anatomical basis for primary abdominal glaucoma. Biometrical comparisons between normal eyes and eyes with primary abdominal glaucoma. Br J Ophthalmol. 1970; 54:161–9.2. Lowe RF. Angle-closure, pupil dilatation, and pupil block. Br J Ophthalmol. 1966; 50:385–9.
Article3. Markowitz SN, Morin JD. The ratio of lens thickness to axial length for biometric standardization in abdominal glaucoma. Am J Ophthalmol. 1985; 99:400–2.4. Marchini G, Pagliarusco A, Toscano A, et al. Ultrasound abdominal and conventional ultrasonographic study of ocular abdominal in primary abdominal glaucoma. Ophthalmology. 1998; 105:2091–8.5. Nongpiur ME, He M, Amerasinghe N, et al. Lens vault, thickness, and position in Chinese subjects with angle closure. Ophthalmology. 2011; 118:474–9.
Article6. Foo LL, Nongpiur ME, Allen JC, et al. Determinants of angle width in Chinese Singaporeans. Ophthalmology. 2012; 119:278–82.
Article7. Aung T, Nolan WP, Machin D, et al. Anterior chamber depth and the risk of primary angle closure in 2 East Asian populations. Arch Ophthalmol. 2005; 123:527–32.
Article8. Alsagoff Z, Aung T, Ang LP, Chew PT. abdominal clinical course of primary abdominal glaucoma in an Asian population. Ophthalmology. 2000; 107:2300–4.9. Robin AL, Pollack IP. Argon laser peripheral iridotomies in the treatment of primary angle closure glaucoma. abdominal fol-low-up. Arch Ophthalmol. 1982; 100:919–23.10. Lam DS, Lai JS, Tham CC, et al. Argon laser peripheral iridoplasty versus conventional systemic medical therapy in treatment of acute primary abdominal glaucoma: a prospective, randomized, abdominalled trial. Ophthalmology. 2002; 109:1591–6.11. Yeung BY, Ng PW, Chiu TY, et al. Prevalence and mechanism of appositional angle closure in acute primary angle closure after iridotomy. Clin Experiment Ophthalmol. 2005; 33:478–82.
Article12. Lam DS, Leung DY, Tham CC, et al. Randomized trial of early phacoemulsification versus peripheral iridotomy to prevent abdominal pressure rise after acute primary angle closure. Ophthalmology. 2008; 115:1134–40.13. Aung T, Ang LP, Chan SP, Chew PT. Acute primary abdominal: long-term intraocular pressure outcome in Asian eyes. Am J Ophthalmol. 2001; 131:7–12.14. Kim DD, Doyle JW, Smith MF. Intraocular pressure reduction abdominal phacoemulsification cataract extraction with posterior chamber lens implantation in glaucoma patients. Ophthalmic Surg Lasers. 1999; 30:37–40.15. Yun YM, Yim JH, Kim CS. Clinical factors that influence abdominal pressure change after cataract surgery in primary open-abdominal glaucoma and abdominal glaucoma. J Korean Ophthalmol Soc. 2006; 47:85–96.16. Sakata LM, Lavanya R, Friedman DS, et al. Comparison of gonioscopy and anterior segment ocular coherence tomography in abdominaling angle closure in different quadrants of the anterior chamber angle. Ophthalmology. 2008; 115:769–74.17. Baskaran M, Ho SW, Tun TA, et al. Assessment of circumferential abdominal by the iris-trabecular contact index with swept-source optical coherence tomography. Ophthalmology. 2013; 120:2226–31.18. Ho SW, Baskaran M, Zheng C, Tun TA. Swept source optical abdominal tomography measurement of the iris-trabecular contact (ITC) index: a new parameter for angle closure. Graefes Arch Clin Exp Ophthalmol. 2013; 251:1205–11.19. Mak H, Xu G, Leung CK. Imaging the iris with swept-source abdominal coherence tomography: relationship between iris volume and primary angle closure. Ophthalmology. 2013; 120:2517–24.20. Moghimi S, Vahedian Z, Fakhraie G, et al. Ocular biometry in the subtypes of angle closure: an anterior segment optical coherence tomography study. Am J Ophthalmol. 2013; 155:664–73. 673.e1.
Article21. Lai I, Mak H, Lai G, et al. Anterior chamber angle imaging with swept-source optical coherence tomography: measuring peripheral anterior synechia in glaucoma. Ophthalmology. 2013; 120:1144–9.
Article22. Lim MC, Lim LS, Gazzard G, et al. Lens opacity, thickness, and position in subjects with acute primary angle closure. J Glaucoma. 2006; 15:260–3.
Article23. Kim YK, Yoo BW, Kim HC, et al. Relative lens vault in subjects with angle closure. BMC Ophthalmol. 2014; 14:93.
Article24. Nongpiur ME, Gong T, Lee HK, et al. Subgrouping of primary abdominal-closure suspects based on anterior segment optical coherence tomography parameters. Ophthalmology. 2013; 120:2525–31.25. Yan YJ, Wu LL, Wang X, Xiao GG. Appositional angle closure in Chinese with primary angle closure and primary angle closure glaucoma after laser peripheral iridotomy. Invest Ophthalmol Vis Sci. 2014; 55:8506–12.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasound Biomicroscopic Changes after Laser Iridotomy or Trabeculectomy in Angle-closure Glaucoma
- Ultrasound biomicroscopic dimensions of the anterior chamber in angle-closure glaucoma patients
- Comparison of Anterior Chamber Depth with Posture Change Between Primary and lens-induced Angle Closure Glaucomas
- Factors Affecting Post-Cataract OCT Parameters in Open-Angle and Angle-Closure Glaucoma Eyes: Optic Disc Head Analysis
- Cataract surgery in patients with acute primary angle-closure glaucoma
