Gastric Mucormycosis Followed by Traumatic Cardiac Rupture in an Immunocompetent Patient
- Affiliations
-
- 1Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu, Korea. lhsworld@nate.com
- KMID: 2350087
- DOI: http://doi.org/10.4166/kjg.2016.68.2.99
Abstract
- Gastric mucormycosis is a rare and life-threatening fungal disease, caused by fungus in the order Mucorales. While rhino-cerebral and pulmonary forms are common, gastric mucormycosis is an uncommon site for the disease. We diagnosed gastric mucormycosis in a 41-year-old female who had severe multiple trauma, including cardiac rupture, due to a traffic accident. Eighteen days after hospitalization, she passed 800 mL of melena over one day. We performed upper esophagogastroduodenoscopy (EGD) and found a huge gastric ulcer with bleeding. Histopathological examination identified non-septated and right-angled branching fungal hyphae, and we diagnosed gastric mucormycosis. We recommended total gastrectomy to her but she refused the operation, so she was treated with liposomal amphotericin B for 53 days. After two months of treatment with liposomal amphotericin B, we again performed EGD and found a healed gastric ulcer. After four months, with another EGD, we found that the gastric mucormycosis was completely healed.
MeSH Terms
Figure
-

Fig. 1. Abdominal CT finding. Irregular gastric wall thickening and air-bubble formation at gastric wall (arrow) were seen. Both pleural effusions were also found.
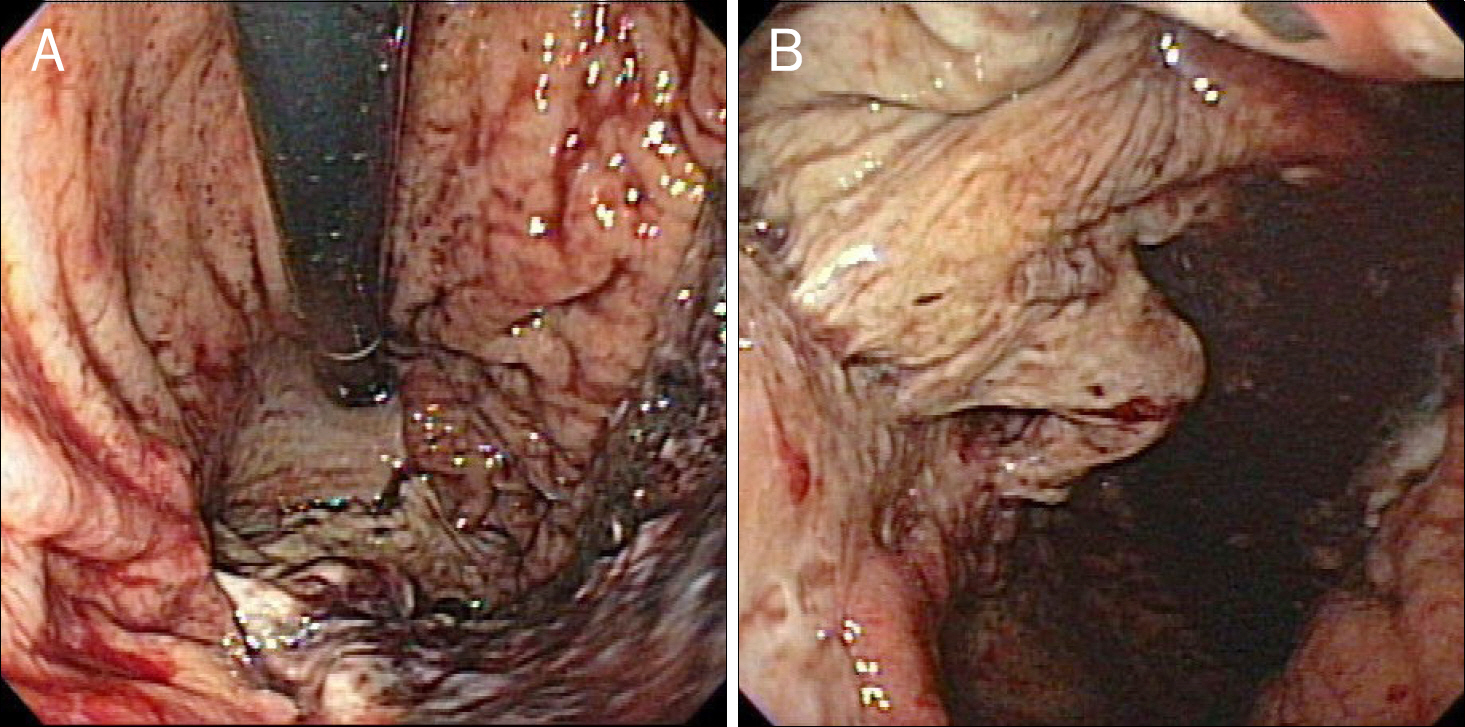
Fig. 2. Endoscopic findings after melena episode. Huge gastric ulcer with bleeding at great curvature side of gastric body and fundus, covered with yellowish exudate.

Fig. 3. Histopathologic findings shown as multiple broad-based, non-septated, right-angle branched fungal hyphae (arrow) with tissue infiltration in H&E (A, ×200), periodic acid-schiff stain (B, ×200), and Gomori methenamine silver stain (C, ×200).

Fig. 4. Endoscopic findings four weeks after starting amphotericin B treatment, showing improving gastric ulcer with surrounding regenerating mucosa at cardia and proximal body.
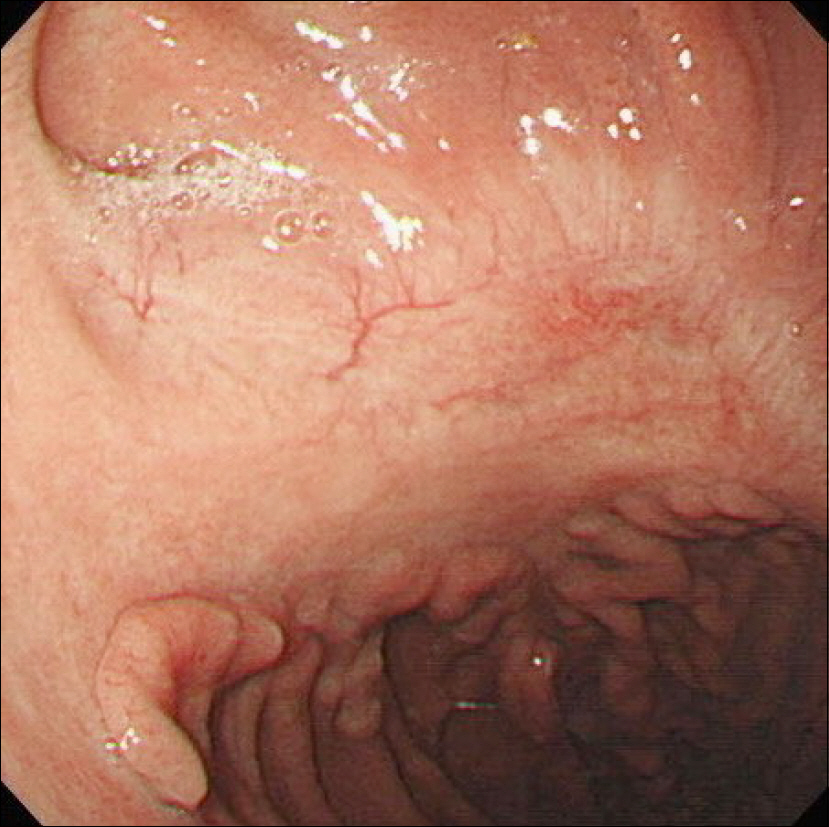
Fig. 5. Endoscopic finding 16 weeks after starting amphotericin B treatment. Gastric ulcer scar formation without rugal fold formation was seen at proximal body.
Reference
-
References
1. Jung JH, Choi HJ, Yoo J, Kang SJ, Lee KY. Emphysematous gastritis associated with invasive gastric mucormycosis: a case report. J Korean Med Sci. 2007; 22:923–927.
Article2. Camara-Lemarroy CR, González-Moreno EI, Rodríguez-Gutiérrez R, et al. Clinical features and outcome of mucormycosis. Interdiscip Perspect Infect Dis. 2014; 2014:562610.
Article3. Ha TS, Park CM, Yang JH, et al. Disseminated gastrointestinal mucormycosis in immunocompromised disease. Korean J Crit Care Med. 2015; 30:323–328.
Article4. Thomson SR, Bade PG, Taams M, Chrystal V. Gastrointestinal mucormycosis. Br J Surg. 1991; 78:952–954.
Article5. Lee JS, Kim HC, Park SW, et al. A case of isolated pulmonary mucormycosis in an immunocompetent host. Tuberc Respir Dis (Seoul). 2013; 74:269–273.
Article6. Pahwa M, Pahwa AR, Girotra M, Chawla A. Isolated renal mucormycosis in a healthy immunocompetent patient: atypical presentation and course. Korean J Urol. 2013; 54:641–643.
Article7. Moon WJ, Kim BJ, Ko YJ, et al. A case of gastric ulcer associated with mucormycosis. Korean J Med. 1999; 56:532–536.8. Shiva Prasad BN, Shenoy A, Nataraj KS. Primary gastrointestinal mucormycosis in an immunocompetent person. J Postgrad Med. 2008; 54:211–213.
Article9. Hahn HS, Jung HS, Song SH, et al. A case intestinal mucormycosis healing of ulcer after only amphotericin B treatment. Korean J Gastrointest Endosc. 2002; 25:43–47.10. Choi WR, Lim CN, Won KH, et al. A case of gastric mucormycosis associated with diabetes mellitus and uremia. Korean J Gastrointest Endosc. 1999; 19:953–958.11. Kim JS, Ko YW, Jang JH, et al. A case of mucormycosis in a patient with myelodysplastic syndrome and review of the literature in Korea. Korean J Infect Dis. 1999; 31:425–434.12. Berne JD, Villarreal DH, McGovern TM, Rowe SA, Moore FO, Norwood SH. A fatal case of posttraumatic gastric mucormycosis. J Trauma. 2009; 66:933–935.
Article13. Johnson CB, Ahmeti M, Tyroch AH, Zuckerman MJ, Hakim MN. Gastric mucormycosis as a cause of life-threatening upper gastrointestinal bleeding in a trauma patient. Am Surg. 2010; 76:E76–E77.
Article14. Stamm B. Mucormycosis of the stomach in a patient with multiple trauma. Histopathology. 2005; 47:222–223.
Article15. Lyon DT, Schubert TT, Mantia AG, Kaplan MH. Phycomycosis of the gastrointestinal tract. Am J Gastroenterol. 1979; 72:379–394.16. Kim J, Lee JH, Byeon JS, Jung HC, Song IS, Kim CY. Gastric mucormycosis in a renal transplant recipient. Korean J Gastrointest Endosc. 1998; 18:230–237.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Primary Cutaneous Mucormycosis in a Immunocompetent Patient
- Primary Cutaneous Mucormycosis Associated with Trauma
- Isolated Renal Mucormycosis in a Healthy Immunocompetent Patient: Atypical Presentation and Course
- Primary Cutaneous Mucormycosis in a Immunocompetent Elderly Woman Showing Sporotrichoid Distribution
- Surgical Treatment of Blunt Traumatic Cardiac Rupture: Two Case Reports
