Preferences and Trends in the Treatment of Diabetic Retinopathy in Korea and Japan
- Affiliations
-
- 1Department of Ophthalmology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. jooeun2@paik.ac.kr
- 2Department of Ophthalmology, Kyungpook National University School of Medicine, Daegu, Korea.
- 3Department of Ophthalmology, Chungnam National University School of Medicine, Daejeon, Korea.
- 4Department of Ophthalmology, Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 5Department of Ophthalmology, Kyung Hee University School of Medicine, Seoul, Korea.
- 6Chang's Retina Center, Daegu, Korea.
- 7Department of Ophthalmology, Korea University College of Medicine, Seoul, Korea.
- 8Department of Ophthalmology, Pusan National University School of Medicine, Yangsan, Korea.
- KMID: 2349071
- DOI: http://doi.org/10.3341/jkos.2016.57.8.1248
Abstract
- PURPOSE
To evaluate preferences and trends in the management of diabetic retinopathy in Korea and Japan.
METHODS
An Internet survey comprised of 49 questions was sent to the members of Korean Retina Society (KRS) and Japanese Society of Ophthalmic Diabetology (JSOD). The survey was conducted during the period between June 2012 and July 2012.
RESULTS
Ninety-one of 210 members of the KRS (43%) and 120 of 754 members of the JSOD (16%) participated in the survey. For diffuse diabetic macular edema, 'intravitreal injection of anti-vascular endothelial growth factor (anti-VEGF) followed by focal laser treatment' was the most preferred treatment in Korea (48%), while 'sub-tenon steroid injection followed by focal laser treatment' was the most common procedure in Japan (33%). Vitrectomy was the second most common procedure in Japan (18%). In contrast, none of the KRS members preferred vitrectomy in this situation. For refractory diabetic macular edema, however, vitrectomy with or without the use of anti-VEGF was chosen in 75% of the KRS members. In Japan, vitrectomy without the use of intravitreal injection of anti-VEGF or steroid was relatively more preferred. Small-gauge (G) vitrectomy using either a 23 G or 25 G needle was popular in both countries (90% in Korea, 64% in Japan).
CONCLUSIONS
Although the trends in diagnostic and surgical environments were similar in Korea and Japan, the preferred treatment approaches for diabetic macular edema were different. Sub-tenon steroid injection and vitrectomy were preferred in Japan, while anti-VEGF injection was most commonly employed in Korea.
MeSH Terms
Figure
-

Figure 1. What is your primary practice setting (%, total N = 91 and 120 in Korea and Japan, respectively)?

Figure 2. How long have you been in practice, after completion of fellowship (%, total N = 91 and 120 in Korea and Japan, respectively)?
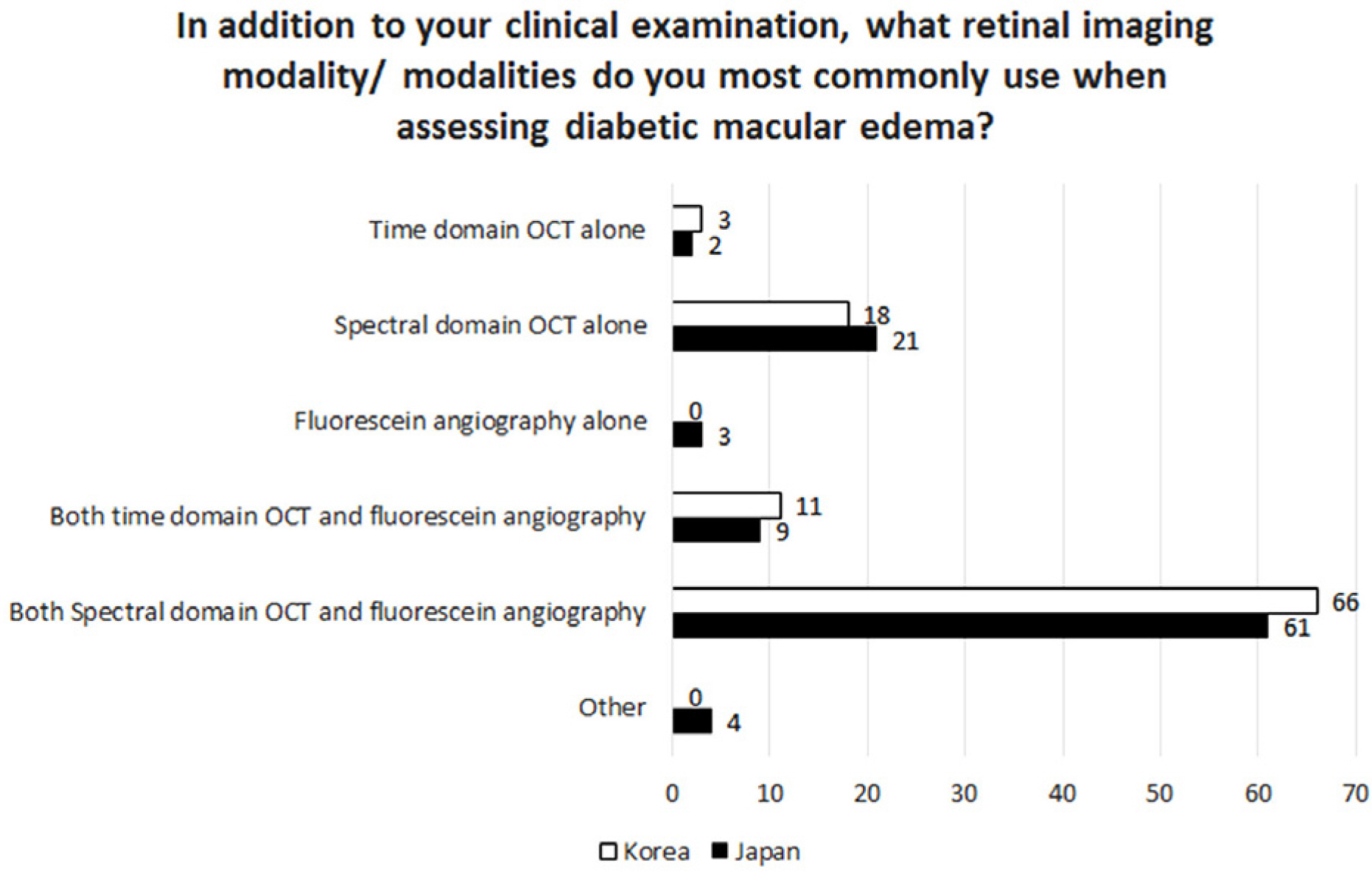
Figure 3. In addition to your clinical examination, what retinal imaging modality/modalities do you most-commonly use when assessing diabetic macular edema (%, total N = 91 and 120 in Korea and Japan, respectively)? OCT = optical coherence tomography.
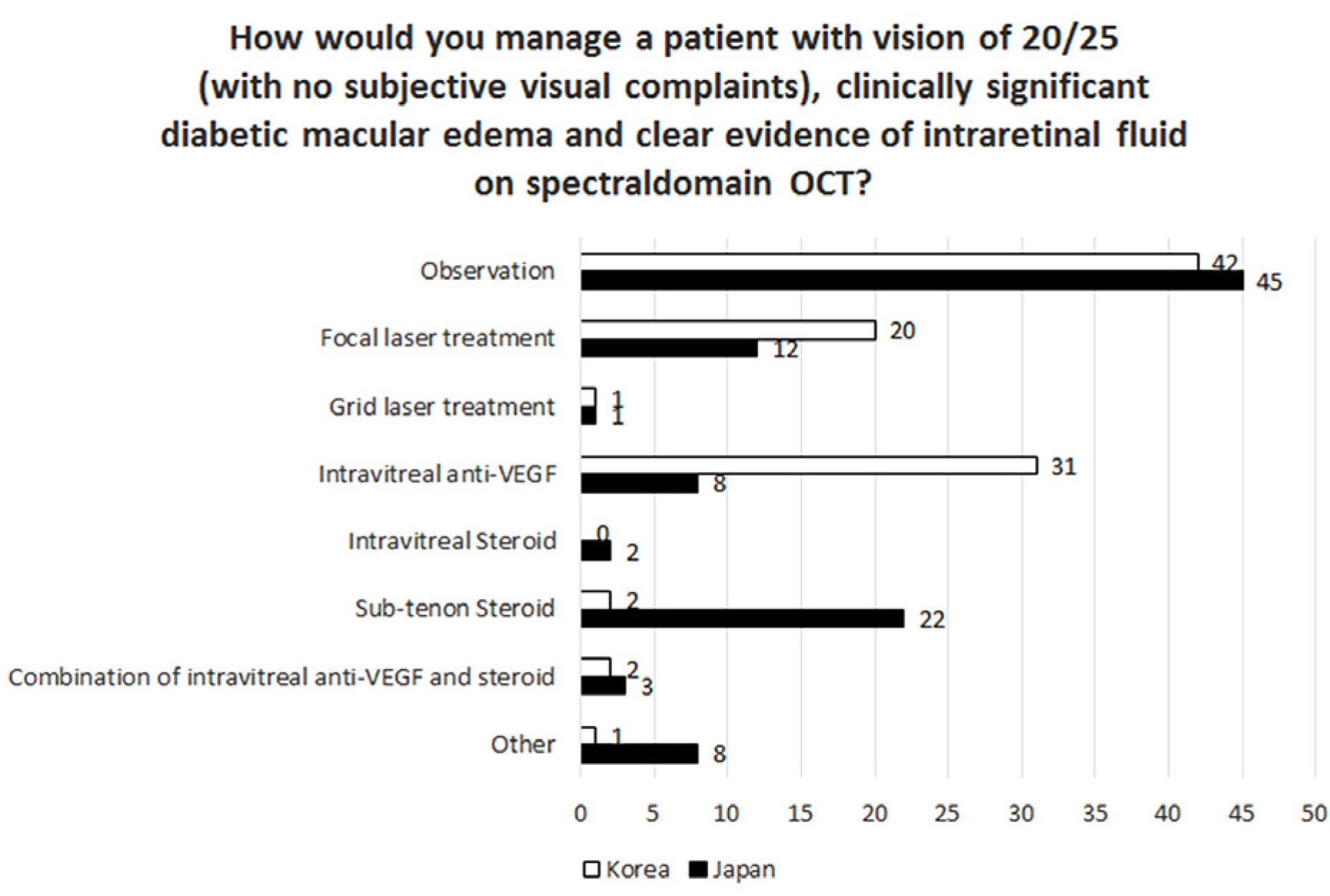
Figure 4. How would you manage a patient with vision of 20/25 (with no subjective visual complaints), clinically significant diabetic macular edema and clear evidence of intraretinal fluid on spectral domain optical coherence tomography (OCT) (%, total N = 91 and 120 in Korea and Japan, respectively)? anti-VEGF = anti-vascular endothelial growth factor.

Figure 5. What combination of therapies do you most commonly use for non-diffuse clinically significant diabetic macular edema (Vision 20/50) (%, total N = 91 and 120 in Korea and Japan, respectively)? anti-VEGF = anti-vascular endothelial growth factor.

Figure 6. What combination of therapies do you most commonly use for diffuse diabetic macular edema (Vision 20/50) (%, total N=91 and 120 in Korea and Japan, respectively)? an-ti-VEGF = anti-vascular endothelial growth factor; Avastin®= Bevacizumab (Genentech, South San Francisco, CA, USA).
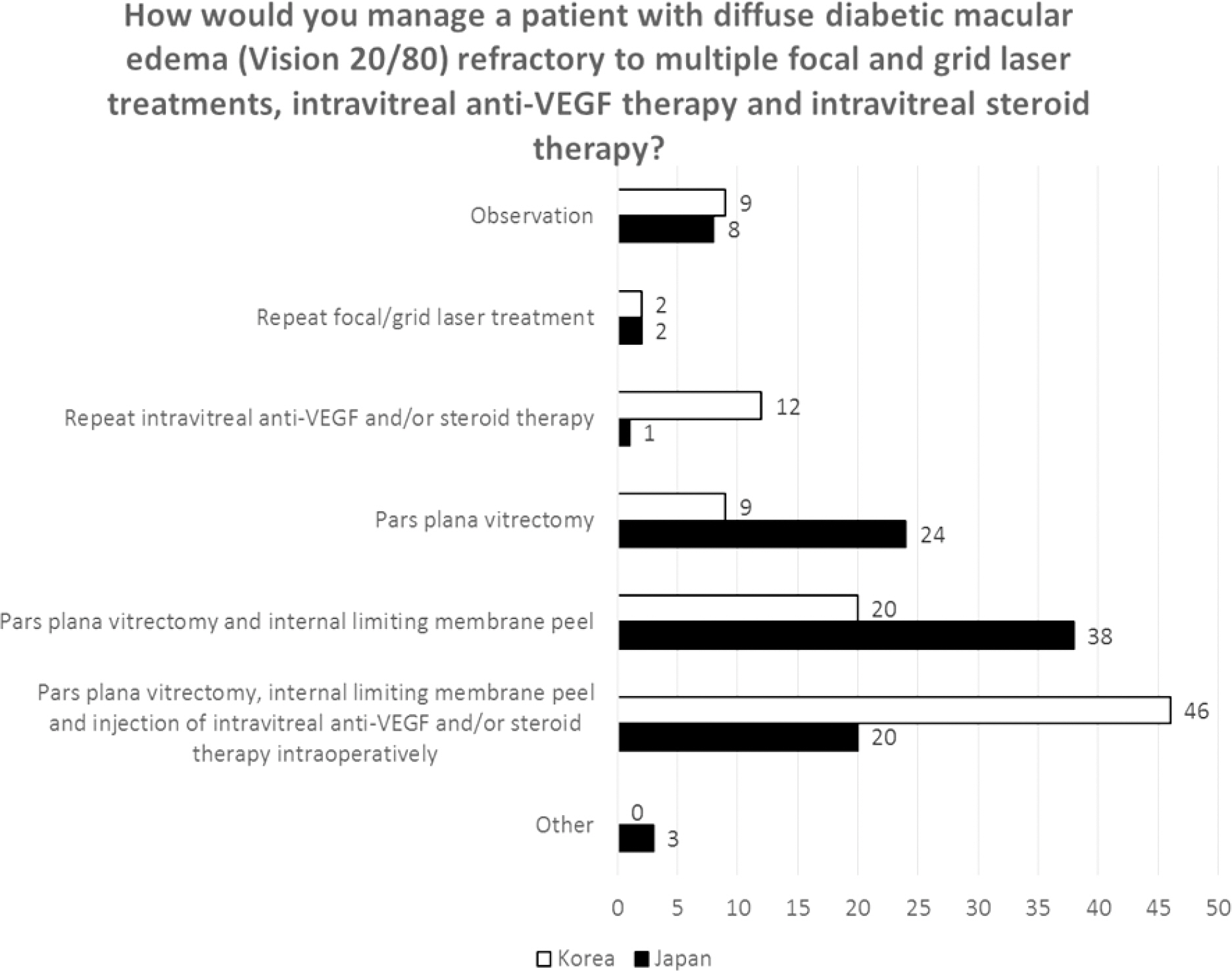
Figure 7. How would you manage a patient with diffuse diabetic macular edema (Vision 20/80) refractory to multiple focal and grid laser treatments, intravitreal anti-VEGF therapy and intravitreal steroid therapy (%, total N=91 and 120 in Korea and Japan, respectively)? anti-VEGF = anti-vascular endothelial growth factor.

Figure 8. Which wavelength do you use most often for pan retinal photocoagulation (PRP) treatment (%, total N=91 and 120 in Korea and Japan, respectively)?

Figure 9. What is your preferred laser treatment method for diffuse diabetic macular edema (with or without combined intravitreal injection of anti-vascular endothelial growth factor [anti-VEGF]) (%, total N=91 and 120 in Korea and Japan, respectively)? ETDRS = Early Treatment of Diabetic Retinopathy Study.
Reference
-
References
1. Yamada M, Hiratsuka Y, Roberts CB, et al. Prevalence of visual impairment in the adult Japanese population by cause and severity and future projections. Ophthalmic Epidemiol. 2010; 17:50–7.
Article2. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Early Treatment Diabetic Retinopathy Study research group. Arch Ophthalmol. 1985; 103:1796–806.3. Boyer DS, Yoon YH, Belfort R Jr, et al. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in abdominals with diabetic macular edema. Ophthalmology. 2014; 121:1904–14.4. Do DV, Schmidt-Erfurth U, Gonzalez VH, et al. The DA VINCI Study: phase 2 primary results of VEGF Trap-Eye in patients with diabetic macular edema. Ophthalmology. 2011; 118:1819–26.
Article5. Michaelides M, Kaines A, Hamilton RD, et al. A prospective randomized trial of intravitreal bevacizumab or laser therapy in the management of diabetic macular edema (BOLT study) 12-month data: report 2. Ophthalmology. 2010; 117:1078–86.e2.6. Mitchell P, Bandello F, Schmidt-Erfurth U, et al. The RESTORE study: ranibizumab monotherapy or combined with laser versus abdominal monotherapy for diabetic macular edema. Ophthalmology. 2011; 118:615–25.7. Nguyen QD, Brown DM, Marcus DM, et al. Ranibizumab for abdominal macular edema: results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology. 2012; 119:789–801.8. Writing Committee for the Diabetic Retinopathy Clinical Research Network. Fong DS, Strauber SF, et al. Comparison of the modified Early Treatment Diabetic Retinopathy Study and mild macular grid laser photocoagulation strategies for diabetic macular edema. Arch Ophthalmol. 2007; 125:469–80.
Article9. Arevalo JF, Sanchez JG, Fromow-Guerra J, et al. Comparison of two doses of primary intravitreal bevacizumab (Avastin) for abdominal diabetic macular edema: results from the Pan-American Collaborative Retina Study Group (PACORES) at 12-month fol-low-up. Graefes Arch Clin Exp Ophthalmol. 2009; 247:735–43.10. Yoon KC, Mun GH, Kim SD, et al. Prevalence of eye diseases in South Korea: data from the Korea National Health and Nutrition Examination Survey 2008–2009. Korean J Ophthalmol. 2011; 25:421–33.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Influences of Arteriosclerosis on the Development and Progression of Diabetic Retinopathy
- New Modalities for the Diagnosis and Treatment of Diabetic Retinopathy
- Clinical Review on Diabetic Retinopathy
- Changes of ERG Parameters in Diabetic Retinopathy
- Photopic Flash ERG Changes in Diabetic Retinopathy: with reference to severity of diabetic retinopathy
