Full-mouth rehabilitation of the patient with severe tooth wear using all ceramic restorations
- Affiliations
-
- 1Department of Prosthodontics, Seoul St. Mary's Hospital, Catholic University of Korea, Seoul, Republic of Korea. lsuyoung@daum.net
- KMID: 2344872
- DOI: http://doi.org/10.4047/jkap.2016.54.3.306
Abstract
- Tooth wear is known as a normal physiological process which gradually progresses. It is reported that vertical dimension can be kept stable because amount of physiologically worn loss could be compensated by growth of alveolar bone and tooth eruption. However, excessive tooth wear as pathologic wear can cause pathologic pulp, disharmony with occlusal plane, functional disorders and esthetic problems so that full mouth rehabilitation could be needed in these cases. Recovery of function and esthetic improvement should be considered for alteration of the vertical dimension. Determination of the vertical dimension of occlusion is needed to be in harmony with the neuromuscular system. This clinical report describes 36 year-old female patient who had chief complaint of severely worn dentition and esthetic discomfort. An increase of 2.0 mm at maxillary incisal edge was done to restore vertical dimension. It was based on the degree of tooth wear and esthetics.
MeSH Terms
Figure
-

Fig. 1. Pre-treatment state. (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Mandibular occlusal view.

Fig. 2. (A) Frontal view of facial photograph before treatment, (B) Panoramic radiograph before treatment.

Fig. 3. (A) Measurement of worn loss, (B) Mounted diagnostic model, (C) An increase of 2.0 mm in vertical dimension.

Fig. 4. Diagnostic wax up. (A) Maxillary occlusal view, (B) Frontal view, (C) Mandibular occlusal view.

Fig. 5. (A) 1st provisional restoration with guideline for modification, (B) 2nd provisional restoration after gingivoplasty, (C) Customized incisal guide table.

Fig. 6. Bisque bake crown after occlusal adjustment. (A) Maxillary occlusal view, (B) Frontal view, (C) Mandibular occlusal view.

Fig. 7. Pre-treatment state. (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Mandibular occlusal view.
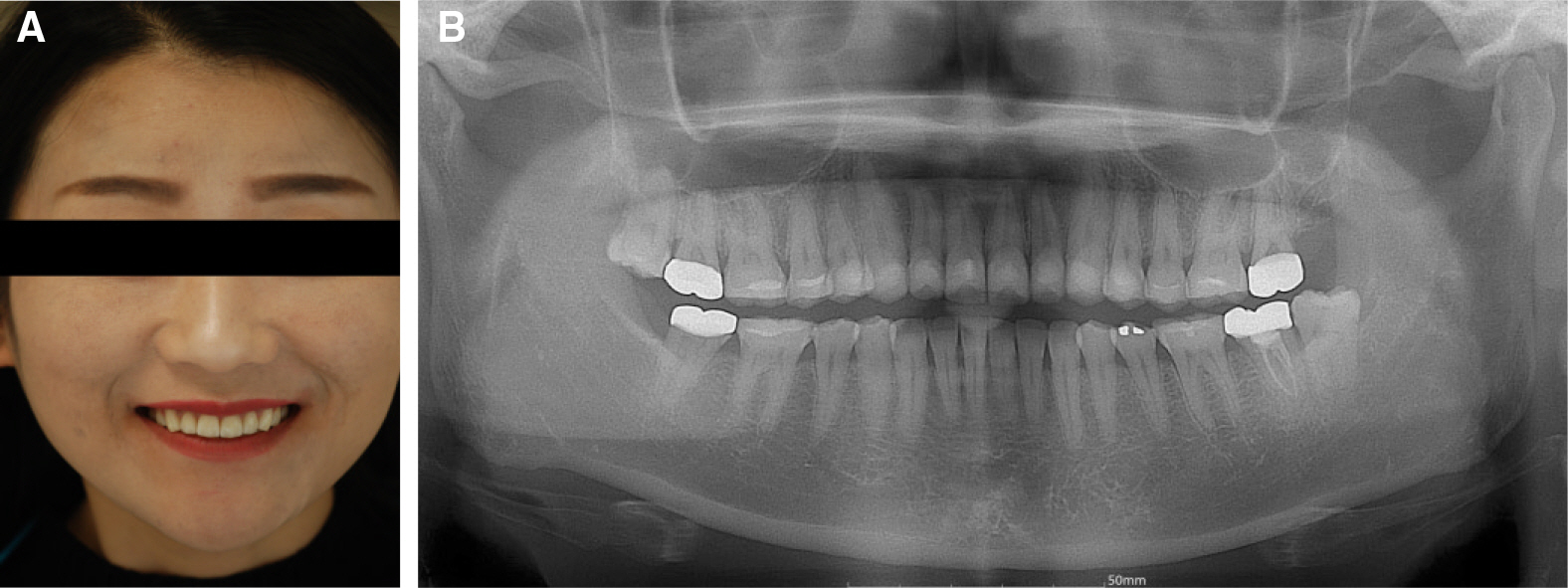
Fig. 8. After treatment state. (A) Frontal view of facial photograph, (B) Panoramic radiograph.
Reference
-
1.Grippo JO., Simring M., Schreiner S. Attrition, abrasion, corrosion and abfraction revisited: a new perspective on tooth surface lesions. J Am Dent Assoc. 2004. 135:1109–18.2.Crothers AJ. Tooth wear and facial morphology. J Dent. 1992. 20:333–41.
Article3.Smith BG., Knight JK. An index for measuring the wear of teeth. Br Dent J. 1984. 156:435–8.
Article4.Lambrechts P., Braem M., Vuylsteke-Wauters M., Vanherle G. Quantitative in vivo wear of human enamel. J Dent Res. 1989. 68:1752–4.
Article5.Ramfjord SP., Blankenship JR. Increased occlusal vertical dimension in adult monkeys. J Prosthet Dent. 1981. 45:74–83.
Article6.Smith BG., Knight JK. A comparison of patterns of tooth wear with aetiological factors. Br Dent J. 1984. 157:16–9.
Article7.Bartlett D., Dugmore C. Pathological or physiological erosion-is there a relationship to age? Clin Oral Investig. 2008. 12:S27–31.
Article8.Donachie MA., Walls AW. The tooth wear index: a flawed epidemiological tool in an ageing population group. Community Dent Oral Epidemiol. 1996. 24:152–8.
Article9.Verrett RG. Analyzing the etiology of an extremely worn dentition. J Prosthodont. 2001. 10:224–33.
Article10.Muts EJ., van Pelt H., Edelhoff D., Krejci I., Cune M. Tooth wear: a systematic review of treatment options. J Prosthet Dent. 2014. 112:752–9.11.Mehta SB., Banerji S., Millar BJ., Suarez-Feito JM. Current concepts on the management of tooth wear: part 1. Assessment, treatment planning and strategies for the prevention and the passive management of tooth wear. Br Dent J. 2012. 212:17–27.
Article12.Mehta SB., Banerji S., Millar BJ., Suarez-Feito JM. Current concepts on the management of tooth wear: part 2. Active restorative care 1: the management of localised tooth wear. Br Dent J. 2012. 212:73–82.
Article13.Mehta SB., Banerji S., Millar BJ., Suarez-Feito JM. Current concepts on the management of tooth wear: part 3. Active restorative care 2: the management of generalised tooth wear. Br Dent J. 2012. 212:121–7.
Article14.Mehta SB., Banerji S., Millar BJ., Suarez-Feito JM. Current concepts on the management of tooth wear: part 4. An overview of the restorative techniques and dental materials commonly applied for the management of tooth wear. Br Dent J. 2012. 212:169–77.
Article15.Turner KA., Missirlian DM. Restoration of the extremely worn dentition. J Prosthet Dent. 1984. 52:467–74.
Article16.Pieger S., Salman A., Bidra AS. Clinical outcomes of lithium disilicate single crowns and partial fixed dental prostheses: a systematic review. J Prosthet Dent. 2014. 112:22–30.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Full mouth rehabilitation of a patient with tooth wear and insufficient restorative space due to loss of posterior teeth support: a case report
- Full mouth rehabilitation with vertical increase in patient with severe tooth wear using monolithic zirconia prosthetic restoration
- Full mouth rehabilitation on the patient with severe tooth wear and tooth fracture using reestabilishment of occlusal vertical dimension
- Full mouth rehabilitation using zirconia crown in severe worn dentition: a case report
- Computer-aided design and manufacturing-based full mouth rehabilitation for a patient with excessive attrition and restricted vertical dimension: A case report
