Korean Circ J.
2016 May;46(3):425-428. 10.4070/kcj.2016.46.3.425.
Non-Bacterial Thrombotic Endocarditis in a Patient with Rheumatoid Arthritis
- Affiliations
-
- 1Department of Rheumatology, Yonsei University Wonju College of Medicine, Wonju, Korea. taeyoung@yonsei.ac.kr
- 2Department of Cardiology, Yonsei University Wonju College of Medicine, Wonju, Korea.
- KMID: 2344458
- DOI: http://doi.org/10.4070/kcj.2016.46.3.425
Abstract
- Rheumatoid arthritis (RA) is frequently associated with various extra-joint complications. Although rare, thromboembolic complications are associated with high morbidity and mortality. We experienced a very rare case of nonbacterial thrombotic endocarditis (NBTE) and subsequent embolic stroke in a patient with RA. A 72-year-old male with a 15-year history of RA suddenly developed neurologic symptoms of vomiting and dizziness. Brain magnetic resonance imaging revealed recently developed multiple cerebellar and cerebral lacunar infarctions. Echocardiography showed a pulsating mitral valve vegetation involving the posterior cusp of the mitral valve leaflet, which was confirmed as NBTE. Immediate anti-coagulation therapy was started. The NBTE lesion disappeared in follow-up echocardiography after 4 weeks of anti-coagulation treatment.
MeSH Terms
Figure
-
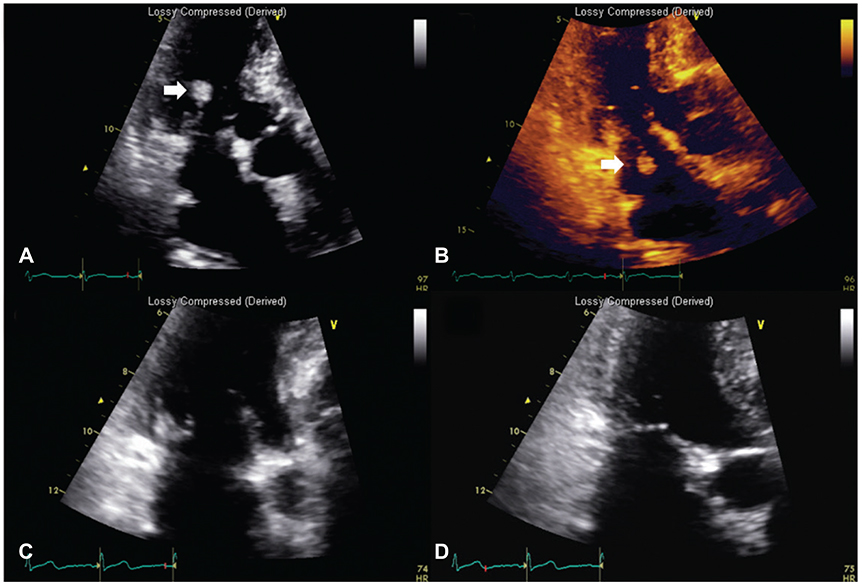
Fig. 1 Mitral valve vegetation. (A, B) Transthoracic echocardiography showing a 0.27×2.27 cm sized characteristic hyperechoic mass-like nodular lesion (NBTE, arrow) attached to the posterior cusp of the mitral valve. This lesion had a stem connecting the mass to the mitral valve, causing the lesion to show a to and fro motion in accordance with the cardiac cycle. (C, D) After 4 weeks of anticoagulation therapy, the NBTE lesion disappeared almost completely on echocardiography. NBTE: nonbacterial thrombotic endocarditis.
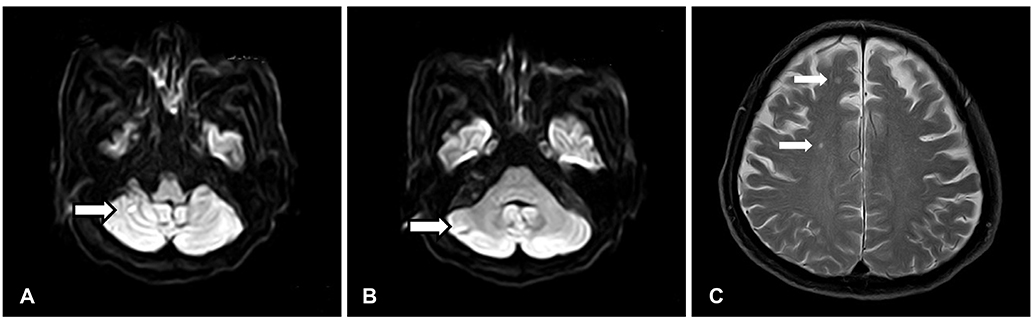
Fig. 2 Brain magnetic resonance image. The arrow indicated the location of multifocal cerebellar (A: diffusion weighted image, B: diffusion weighted image) and cerebral infarctions (C: T2 weighted image).
Reference
-
1. Eiken PW, Edwards WD, Tazelaar HD, McBane RD, Zehr KJ. Surgical pathology of nonbacterial thrombotic endocarditis in 30 patients, 1985-2000. Mayo Clin Proc. 2001; 76:1204–1212.2. Meune C, Touzé E, Trinquart L, Allanore Y. Trends in cardiovascular mortality in patients with rheumatoid arthritis over 50 years: a systematic review and meta-analysis of cohort studies. Rheumatology (Oxford). 2009; 48:1309–1313.3. Solomon DH, Karlson EW, Rimm EB, et al. Cardiovascular morbidity and mortality in women diagnosed with rheumatoid arthritis. Circulation. 2003; 107:1303–1307.4. el-Shami K, Griffiths E, Streiff M. Nonbacterial thrombotic endocarditis in cancer patients: pathogenesis, diagnosis, and treatment. Oncologist. 2007; 12:518–523.5. Turiel M, Sitia S, Atzeni F, et al. The heart in rheumatoid arthritis. Autoimmun Rev. 2010; 9:414–418.6. Wislowska M, Sypula S, Kowalik I. Echocardiographic findings, 24-hour electrocardiographic Holter monitoring in patients with rheumatoid arthritis according to Steinbrocker's criteria, functional index, value of Waaler-Rose titre and duration of disease. Clin Rheumatol. 1998; 17:369–377.7. Aviña-Zubieta JA, Choi HK, Sadatsafavi M, Etminan M, Esdaile JM, Lacaille D. Risk of cardiovascular mortality in patients with rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum. 2008; 59:1690–1697.8. Baghdadi LR, Woodman RJ, Shanahan EM, Mangoni AA. The impact of traditional cardiovascular risk factors on cardiovascular outcomes in patients with rheumatoid arthritis: a systematic review and meta-analysis. PLoS One. 2015; 10:e0117952.9. Kim SC, Solomon DH, Liu J, Franklin JM, Glynn RJ, Schneeweiss S. Risk of venous thromboembolism in patients with rheumatoid arthritis: initiating disease-modifying antirheumatic drugs. Am J Med. 2014; 128:539.e7–539.e17.10. Chatzis A, Giannopoulos N, Baharakakis S, Saridakis N, Agapitos E, Stamatelopoulos S. Unusual cause of a stroke in a patient with seronegative rheumatoid arthritis. Cardiovasc Surg. 1999; 7:659–660.11. Mounet F, Soula P, Concina P, Baradat G, Céréne A. [Heart valve diseases specific in rheumatoid polyarthritis. Apropos of 2 cases]. Arch Mal Coeur Vaiss. 1997; 90:987–989.12. Kang H, Baron M. Embolic complications of a mitral valve rheumatoid nodule. J Rheumatol. 2004; 31:1001–1003.13. Choi HK, Rho YH, Zhu Y, Cea-Soriano L, Aviña-Zubieta JA, Zhang Y. The risk of pulmonary embolism and deep vein thrombosis in rheumatoid arthritis: a UK population-based outpatient cohort study. Ann Rheum Dis. 2013; 72:1182–1187.14. Bacani AK, Gabriel SE, Crowson CS, Heit JA, Matteson EL. Noncardiac vascular disease in rheumatoid arthritis: increase in venous thromboembolic events? Arthritis Rheum. 2012; 64:53–61.15. van der Poll T, Büller HR, ten Cate H, et al. Activation of coagulation after administration of tumor necrosis factor to normal subjects. N Engl J Med. 1990; 322:1622–1627.16. Ong ML, Veerapen K, Chambers JB, Lim MN, Manivasagar M, Wang F. Cardiac abnormalities in systemic lupus erythematosus: prevalence and relationship to disease activity. Int J Cardiol. 1992; 34:69–74.17. Mazokopakis EE, Syros PK, Starakis IK. Nonbacterial thrombotic endocarditis (marantic endocarditis) in cancer patients. Cardiovasc Hematol Disord Drug Targets. 2010; 10:84–86.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Non-Infective Endocarditis in a Patient with Rheumatoid Arthritis
- A Case of Pneumococcal Endocarditis Accompanied by Arthritis and Meningitis
- An autopsy case of nonbacterial thrombotic endocarditis
- Cytokines in rheumatoid arthritis
- Clinical significance of rheumatoid factor in juvenile rheumatoid arthritis
