Central Decompressive Laminoplasty for Treatment of Lumbar Spinal Stenosis : Technique and Early Surgical Results
- Affiliations
-
- 1Department of Neurosurgery, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. neuriac@skku.edu
- KMID: 2339958
- DOI: http://doi.org/10.3340/jkns.2014.56.3.206
Abstract
OBJECTIVE
Lumbar spinal stenosis is a common degenerative spine disease that requires surgical intervention. Currently, there is interest in minimally invasive surgery and various technical modifications of decompressive lumbar laminectomy without fusion. The purpose of this study was to present the author's surgical technique and results for decompression of spinal stenosis.
METHODS
The author performed surgery in 57 patients with lumbar spinal stenosis between 2006 and 2010. Data were gathered retrospectively via outpatient interviews and telephone questionnaires. The operation used in this study was named central decompressive laminoplasty (CDL), which allows thorough decompression of the lumbar spinal canal and proximal two foraminal nerve roots by undercutting the lamina and facet joint. Kyphotic prone positioning on elevated curvature of the frame or occasional use of an interlaminar spreader enables sufficient interlaminar working space. Pain was measured with a visual analogue scale (VAS). Surgical outcome was analyzed with the Oswestry Disability Index (ODI). Data were analyzed preoperatively and six months postoperatively.
RESULTS
The interlaminar window provided by this technique allowed for unhindered access to the central canal, lateral recess, and upper/lower foraminal zone, with near-total sparing of the facet joint. The VAS scores and ODI were significantly improved at six-month follow-up compared to preoperative levels (p<0.001, respectively). Excellent pain relief (>75% of initial VAS score) of back/buttock and leg was observed in 75.0% and 76.2% of patients, respectively.
CONCLUSION
CDL is easily applied, allows good field visualization and decompression, maintains stability by sparing ligament and bony structures, and shows excellent early surgical results.
Keyword
MeSH Terms
Figure
-
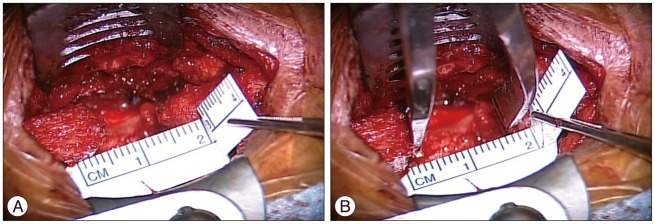
Fig. 1 Intraoperative findings during interlaminar window exposure. A : In the beginning of the exposure, narrow interspinous distance (about 1cm) is noted after removal of small portion of spinous process. B : Gradual retraction using bony spreader between spinous processes in kyphotic prone position provides wider surgical window.
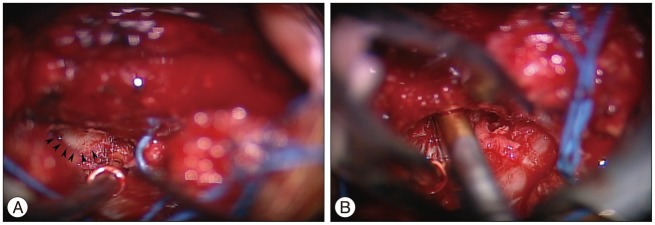
Fig. 2 Intraoperative findings during removal of the tip of the superior articular process. A : Tilting down the table toward the opposite side provides the surgical view to expose the tip of the superior articular process (arrowheads). B : Decompression from contralateral side enables removal of the tip and widening of the neural foramen without disruptions of overlying inferior articular process and facet capsule.
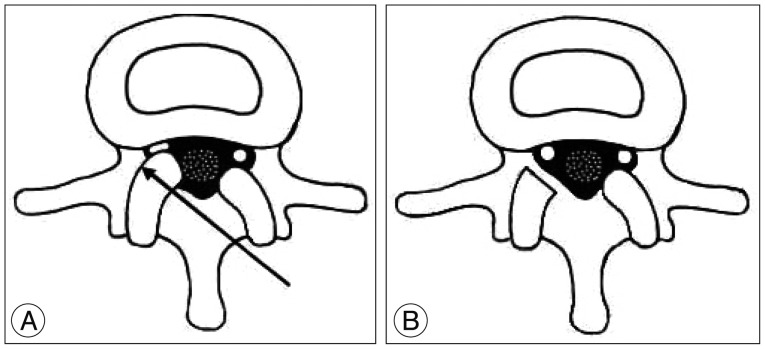
Fig. 3 Decompression of a traversing root via contralateral trajectory. Compressed root by hypertrophied articular processes (A) can be decompressed by inclined undercutting removal without disruption of facet joint and overlying capsule (B).
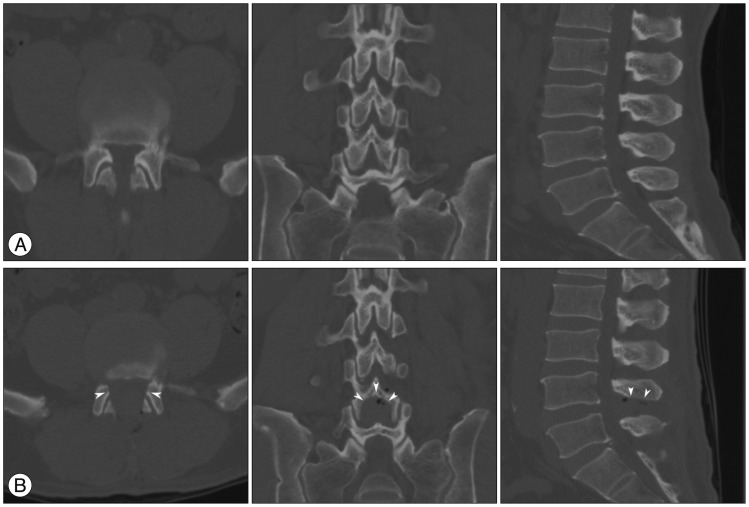
Fig. 4 Pre (A)- and post (B)-operative CT findings in a surgical patient. Angular shaped undercutting of facet joint to the pedicle is performed (left). Undercutting of the internal portion of the L4 lamina (arrowheads) is noted in coronal (middle) and sagittal (right) plane.
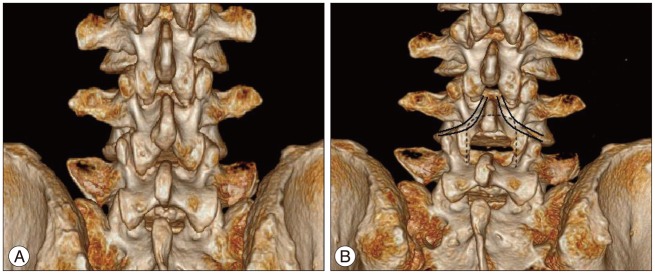
Fig. 5 Pre (A)- and post (B)-operative 3D reconstructed CT. Postoperative view (B) reveals spared portions of spinous process, lamina, and facet, compared with preoperative view (A). Postoperative view shows wide decompressed bony window including central laminoplasty area (delineated by dotted line), which decompresses proximal exiting roots and preserves facet joints.
Reference
-
1. Abumi K, Panjabi MM, Kramer KM, Duranceau J, Oxland T, Crisco JJ. Biomechanical evaluation of lumbar spinal stability after graded facetectomies. Spine (Phila Pa 1976). 1990; 15:1142–1147. PMID: 2267608.
Article2. Adams MA, Hutton WC. The mechanical function of the lumbar apophyseal joints. Spine (Phila Pa 1976). 1983; 8:327–330. PMID: 6623200.
Article3. Adams MA, Hutton WC, Stott JR. The resistance to flexion of the lumbar intervertebral joint. Spine. 1980; 5:245–253. PMID: 7394664.
Article4. Aryanpur J, Ducker T. Multilevel lumbar laminotomies : an alternative to laminectomy in the treatment of lumbar stenosis. Neurosurgery. 1990; 26:429–432. discussion 433. PMID: 2138716.5. Cavuşoğlu H, Kaya RA, Türkmenoglu ON, Tuncer C, Colak I, Aydin Y. Midterm outcome after unilateral approach for bilateral decompression of lumbar spinal stenosis : 5-year prospective study. Eur Spine J. 2007; 16:2133–2142. PMID: 17712577.
Article6. Getty CJ, Johnson JR, Kirwan EO, Sullivan MF. Partial undercutting facetectomy for bony entrapment of the lumbar nerve root. J Bone Joint Surg Br. 1981; 63-B:330–335. PMID: 7263743.
Article7. Haher TR, O'Brien M, Dryer JW, Nucci R, Zipnick R, Leone DJ. The role of the lumbar facet joints in spinal stability. Identification of alternative paths of loading. Spine (Phila Pa 1976). 1994; 19:2667–2670. discussion 2671. PMID: 7899961.8. Herron LD, Pheasant HC. Bilateral laminotomy and discectomy for segmental lumbar disc disease. Decompression with stability. Spine (Phila Pa 1976). 1983; 8:86–97. PMID: 6867860.9. Jang JW, Park JH, Hyun SJ, Rhim SC. Clinical outcomes and radiologic changes following microsurgical bilateral decompression via a unilateral approach in patients with lumbar canal stenosis and grade I degenerative spondylolisthesis with a minimum 3-year follow-up. J Spinal Disord Tech. 2012; [Epub ahead of print].10. Jeon CH, Kim DJ, Kim DJ, Lee HM, Park HJ. Cross-cultural adaptation of the Korean Version Of the Oswestry Disability Index (ODI). J Korean Soc Spine Surg. 2005; 12:146–152.
Article11. Ji YC, Kim YB, Hwang SN, Park SW, Kwon JT, Min BK. Efficacy of unilateral laminectomy for bilateral decompression in elderly lumbar spinal stenosis. J Korean Neurosurg Soc. 2005; 37:410–415.12. Johnsson KE, Redlund-Johnell I, Udén A, Willner S. Preoperative and postoperative instability in lumbar spinal stenosis. Spine (Phila Pa 1976). 1989; 14:591–593. PMID: 2749373.
Article13. Jönsson B, Annertz M, Sjöberg C, Strömqvist B. A prospective and consecutive study of surgically treated lumbar spinal stenosis. Part II : Five-year follow-up by an independent observer. Spine (Phila Pa 1976). 1997; 22:2938–2944. PMID: 9431630.
Article14. Katz JN, Lipson SJ, Larson MG, McInnes JM, Fossel AH, Liang MH. The outcome of decompressive laminectomy for degenerative lumbar stenosis. J Bone Joint Surg Am. 1991; 73:809–816. PMID: 2071616.
Article15. Lin SM, Tseng SH, Yang JC, Tu CC. Chimney sublaminar decompression for degenerative lumbar spinal stenosis. J Neurosurg Spine. 2006; 4:359–364. PMID: 16703902.
Article16. Poletti CE. Central lumbar stenosis caused by ligamentum flavum : unilateral laminotomy for bilateral ligamentectomy : preliminary report of two cases. Neurosurgery. 1995; 37:343–347. PMID: 7477792.17. Sanderson PL, Getty CJ. Long-term results of partial undercutting facetectomy for lumbar lateral recess stenosis. Spine (Phila Pa 1976). 1996; 21:1352–1356. PMID: 8725928.
Article18. Scholz M, Firsching R, Lanksch WR. Long-term follow up in lumbar spinal stenosis. Spinal Cord. 1998; 36:200–204. PMID: 9554022.19. Spetzger U, Bertalanffy H, Naujokat C, von Keyserlingk DG, Gilsbach JM. Unilateral laminotomy for bilateral decompression of lumbar spinal stenosis. Part I : Anatomical and surgical considerations. Acta Neurochir (Wien). 1997; 139:392–396. PMID: 9204106.
Article20. Thomas NW, Rea GL, Pikul BK, Mervis LJ, Irsik R, McGregor JM. Quantitative outcome and radiographic comparisons between laminectomy and laminotomy in the treatment of acquired lumbar stenosis. Neurosurgery. 1997; 41:567–574. discussion 574-575. PMID: 9310973.
Article21. Tuite GF, Stern JD, Doran SE, Papadopoulos SM, McGillicuddy JE, Oyedijo DI, et al. Outcome after laminectomy for lumbar spinal stenosis. Part I : Clinical correlations. J Neurosurg. 1994; 81:699–706. PMID: 7755690.22. Watanabe K, Hosoya T, Shiraishi T, Matsumoto M, Chiba K, Toyama Y. Lumbar spinous process-splitting laminectomy for lumbar canal stenosis. Technical note. J Neurosurg Spine. 2005; 3:405–408. PMID: 16302638.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Long-term Clinical and Radiological Outcomes after Central Decompressive Laminoplasty for Lumbar Spinal Stenosis
- Unilateral Undercutting Laminoplasty in the Treatment of Lumbar Spinal Stenosis: Comparison with Conventional Bilateral Partial Laminectomy
- Transpedicular Screw instrumentation and Spinal Fusion after Laminectomy in Lumbar Spinal Stenosis
- Minimally Invasive Combined Interlaminar and Paraisthmic Approach for Symptomatic Lumbar Foraminal Stenosis : Surgical Technique and Preliminary Results
- A Case of Coexisting Cervical and Lumbar Spinal Stenosis
