J Korean Ophthalmol Soc.
2014 Jun;55(6):918-922.
A Case of Corneal Ulcer Caused by Leclercia Adecarboxylata
- Affiliations
-
- 1Department of Ophthalmology and Visual Science, The Catholic University of Korea College of Medicine, Seoul, Korea. leoanzel@catholic.ac.kr
Abstract
- PURPOSE
To report a case of corneal ulcer caused by Leclercia adecarboxylata in an immunocompetent patient.
CASE SUMMARY
A previously healthy 43-year-old female presented with right ocular pain and was referred to our clinic under the impression of corneal abrasion and secondary infection. The patient was treated at a local clinic for 3 days using artificial tears, therapeutic contact lens, topical antibiotics, and anti-inflammatory eye drops but showed no improvement. Gram staining, bacterial and fungal cultures and antibiotic sensitivity test were performed from a corneal scrape. The cultures revealed growth of Leclercia adecarboxylata. The patient was treated with moxifloxacin and ofloxacin eye drops. After 2 weeks of treatment, the infection resolved without remaining scars.
CONCLUSIONS
Reportedly, Leclercia adecarboxylata affects humans only as an opportunistic pathogen or part of polymicrobial infections. However, in the present case, Leclercia adecarboxylata was isolated as a single pathogen in an immunocompetent patient which is the first clinical report of this microorganism found in an ocular sample. Therefore, if antibiotic-susceptible gram-negative bacilli are found in opthalmologic samples, the above bacteria should be considerd in the diagnosis.
MeSH Terms
Figure
-
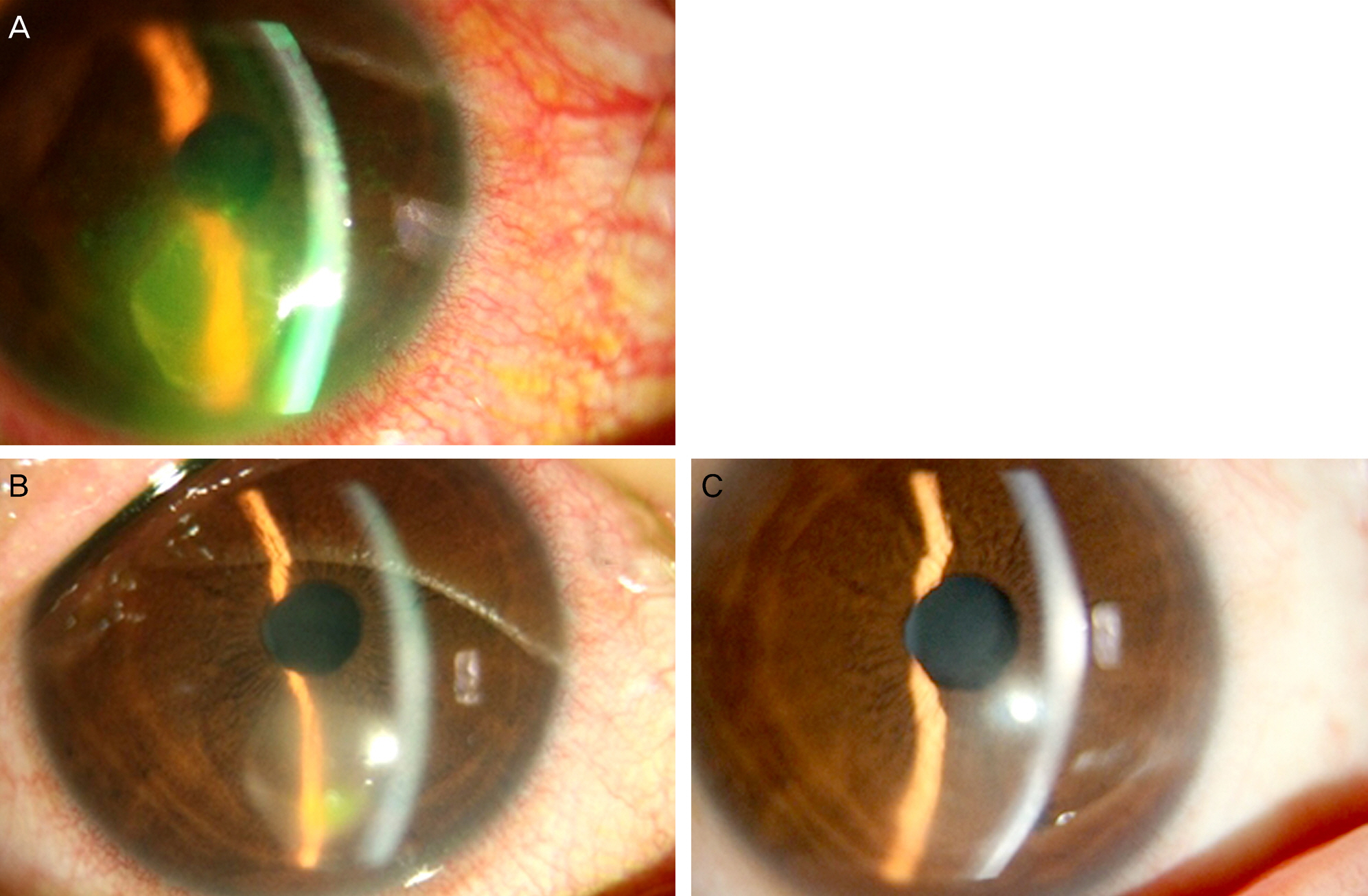
Figure 1. (A) Anterior segment photograph at the first oph-thalmic examination showing a corneal ulcer with deep stromal infiltrations and linear hypopyon. (B) Corneal ulcer with de-creased stromal infiltration and remaining hypopyon on the 2nd day of antibacterial treatment. (C) Nearly regressed corneal ul-cer on the 7th day of antibacterial treatment.
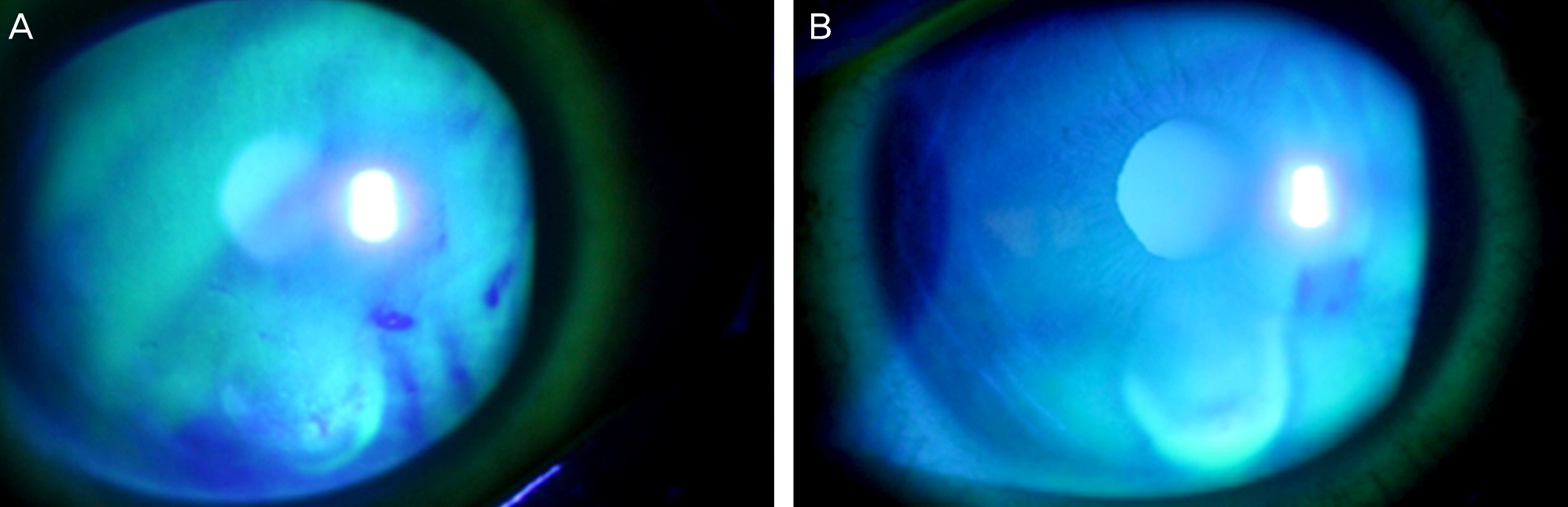
Figure 2. (A) Anterior segment photograph (Fluorescein dye stained) on the 3rd day after starting anti-bacterial treatment; better marginated corneal ulcer with decreased stromal infiltration. (B) Anterior segment photograph (Fluorescein dye stained) on the 5th day showing decreased epithelial defects with remnant bacterial collections at the inferior cornea.
Reference
-
References
1. Lecler H. Etude biochemique d'enterobacteriaceae pigmentees. Ann Inst Pasteur. 1962; 102:726–41.2. Richard C. New Enterobacteriaceae found in medical bacteriology Moellerella wisconsensis, Koserella trabulsii, Leclercia adecarbox-ylata, Escherichia fergusonii, Enterobacter asbutiae, Rahnella aquatilis. Ann Biol Clin (Paris). 1989; 47:231–6.3. Tamura K, Sakazaki R, Kosako Y, Yoshizaki E. Leclercia ade-carboxylata gen. nov., comb. nov., formerly known as Escherichia adecarboxylata. Curr Microbiol. 1986; 13:179–84.4. Hwang HY, Jeong SH, Rim H, et al. A case of Leclercia adecarbox-ylata isolated from dialysate in a patient with continuous ambula-tory peritoneal dialysis. Korean J Clin Microbiol. 1998; 1:113–6.5. Mazzariol A, Zuliani J, Fontana R, Cornaglia G. Isolation from blood culture of a Leclercia adecarboxylata strain producing an SHV-12 extended-spectrum beta-lactamase. J Clin Microbiol. 2003; 41:1738–9.6. Dalamaga M, Pantelaki M, Papadavid E, et al. Epididymo-orchitis and bacteremia caused by Leclercia adecarboxylata. Med Mal Infect. 2008; 38:674–5.7. Dalamaga M, Pantelaki M, Karmaniolas K, et al. Isolation of Leclercia adecarboxylata from blood and burn wound after a hy-drofluoric acid chemical injury. Burns. 2009; 35:443–5.
Article8. Davenport P, Land KJ. Isolation of Leclercia adecarboxylata from the blood culture of an asymptomatic platelet donor. Transfusion. 2007; 47:1816–9.
Article9. Sawamura H, Kawamura Y, Yasuda M, et al. A clinical isolate of Leclercia adecarboxylata from a patient of pyelonephritis. Kansenshogaku Zasshi. 2005; 79:831–5.
Article10. Beltrán A, Molinero AV, Capilla S, et al. Isolation of Leclercia ade-carboxylata from wound exudate of a diabetic patient. Med Clin (Barc). 2004; 122:159.11. Pérez-Moreno MO, Anguera J, Carulla M, Pérez-Moreno M. Septic arthritis due to Leclercia adecarboxylata of probable iatro-genic origin. Enferm Infecc Microbiol Clin. 2003; 21:167–8.12. Jover-Sáenz A, Cerezo-Esforzado E, Barcenilla-Gaite F, et al. Leclercia adecarboxylata cholecystitis in a patient with metabolic syndrome. Surg Infect (Larchmt). 2008; 9:411–2.
Article13. Rodríguez JA, Sánchez FJ, Gutiérrez N, et al. Bacterial peritonitis due to Leclercia adecarboxylata in a patient undergoing peritoneal dialysis. Enferm Infecc Microbiol Clin. 2001; 19:237–8.14. Longhurst CA, West DC. Isolation of Leclercia adecarboxylata from an infant with acute lymphoblastic leukemia. Clin Infect Dis. 2001; 32:1659.
Article15. de Baere T, Wauters G, Huylenbroeck A, et al. Isolations of Leclercia adecarboxylata from a patient with a chronically in-flamed gallbladder and from a patient with sepsis without focus. J Clin Microbiol. 2001; 39:1674–5.16. Fattal O, Deville JG. Leclercia adecarboxylata peritonitis in a child receiving chronic peritoneal dialysis. Pediatr Nephrol. 2000; 15:186–7.
Article17. Temesgen Z, Toal DR, Cockerill FR 3rd. Leclercia adecarboxylata infections: case report and review. Clin Infect Dis. 1997; 25:79–81.18. Lee NY, Ki CS, Kang WK, et al. Hickman catheter-associated bac-teremia by Leclercia adecarboxylata and Escherichia hermannii: a case report. Korean J Infect Dis. 1999; 31:167–70.19. Bali R, Sharma P, Gupta K, Nagrath S. Pharyngeal and peritonsillar abscess due to Leclercia adecarboxylata in an immunocompetant patient. Journal of Infection in Developing Countries. 2013; 7:46–50.
Article20. Daza RM, Iborra J, Alonso N, et al. Isolation of Leclercia ade-carboxylata in a cirrhotic patient. Enferm Infecc Microbiol Clin. 1993; 11:53–4.21. Oldenburg CE, Lalitha P, Srinivasan M, et al. Moxifloxacin sus-ceptibility mediates the relationship between causative organism and clinical outcome in bacterial keratitis. Invest Ophthalmol Vis Sci. 2013; 54:1522–6.
Article22. Sharma N, Goel M, Bansal S, et al. Evaluation of moxifloxacin 0.5% in treatment of nonperforated bacterial corneal ulcers: a randomized controlled trial. Ophthalmology. 2013; 120:1173–8.23. Kim MJ, Yu F, Aldave AJ. Microbial keratitis after Boston Type I keratoprosthesis implantation: incidence, organisms, risk factors, and outcomes. Ophthalmology. 2013; 120:2209–16.24. Hess B, Burchett A, Huntington MK. Leclercia adecarboxylata in an immunocompetent patient. J Med Microbiol. 2008; 57:896–8.
Article25. Stock I, Burak S, Wiedemann B. Natural antimicrobial suscepti-bility patterns and biochemical profiles of Leclercia adecarbox-ylata strains. Clinical Microbiology and Infection. 2004; 10:724–33.
Article26. Ferrari TM, Leozappa M, Lorusso M, et al. Escherichia coli kerati-tis treated with ultraviolet A/riboflavin corneal cross-linking: a case report. Eur J Ophthalmol. 2009; 19:295–297.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Leclercia adecarboxylata Infection Following Wood Stick Injury
- Two Cases of Independent Infection by Leclercia adecarboxylata
- A Case of Diabetic Foot Infection due to Leclercia adecarboxylata
- Hickman Catheter-Associated Bacteremia by Leclercia adecarboxylata and Escherichia hermannii: A Case Report
- Pseudobacteremic Outbreak of Leclercia adecarboxylata and Pseudomons aeruginosa Related to Contaminated Saline Cotton
