Correlation between Foveal Thickness and Visual Acuity in Unilateral Resolved Central Serous Chorioretinopathy
- Affiliations
-
- 1Department of Ophthalmology, Gyeongsang National University, College of Medicine, Chinju, Korea. sjk@nongae.ac.kr
Abstract
-
PURPOSE: To evaluate the correlation between foveal thickness, as measured with optical coherence tomographic evaluation, and the visual acuity in patients who suffered from unilateral resolved central serous chorioretinopathy.
METHODS
Twenty-eight consecutive patients who were diagnosed with unilateral resolved central serous chorioretinopathy were studied. High-resolution optical coherence tomography was performed on all of the patients. The foveal thickness of the involved eye was normalized by dividing its thickness with that of the uninvolved eye. The best-corrected visual acuity of the involved eye was normalized as well. The subjects were divided into two groups according to the minimum value of the normalized foveal thickness in the 22 healthy subjects.
RESULTS
The mean foveal thickness was 128.68+/-22.06 micrometer in the involved eyes and 148.18+/-13.88 micrometer in the uninvolved eyes. There was a statistically significant correlation between the normalized foveal thickness and the normalized visual acuity. There were statistically significant differences in the normalized visual acuity and the duration of the symptoms between the group with foveal thickness above the minimum value and the group with foveal thickness below the minimum value.
CONCLUSIONS
There was a statistically significant correlation between foveal thickness and visual acuity. The patient group with a foveal thickness value above the minimum value of the normalized foveal thickness showed a statistically significant improvement in visual acuity and a shorter duration of symptoms. It seems that the foveal thickness is associated with visual acuity and the duration of symptoms.
Figure
-
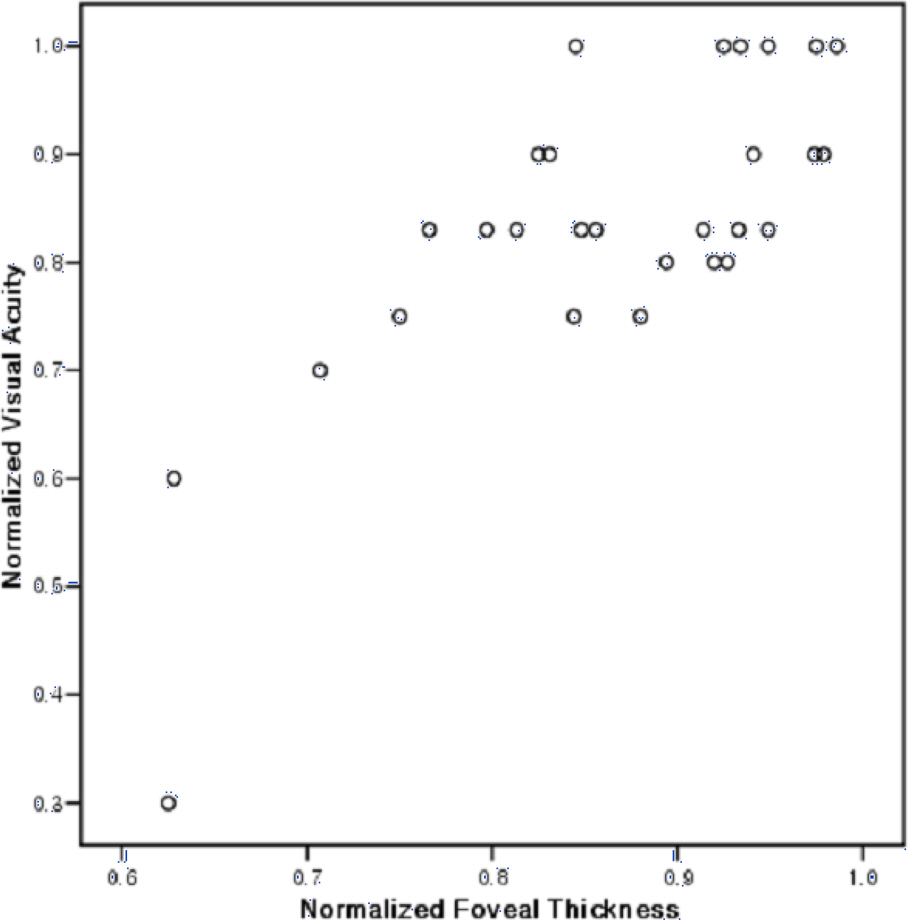
Figure 1. The normalized visual acuity, which was calculated by dividing the visual acuity of the involved eye by that of the uninvolved eye (expressed as a proportion), was plotted against the normalized foveal thickness, also expressed as a proportion (r=0.756, p<0.05, two-sample t-test).
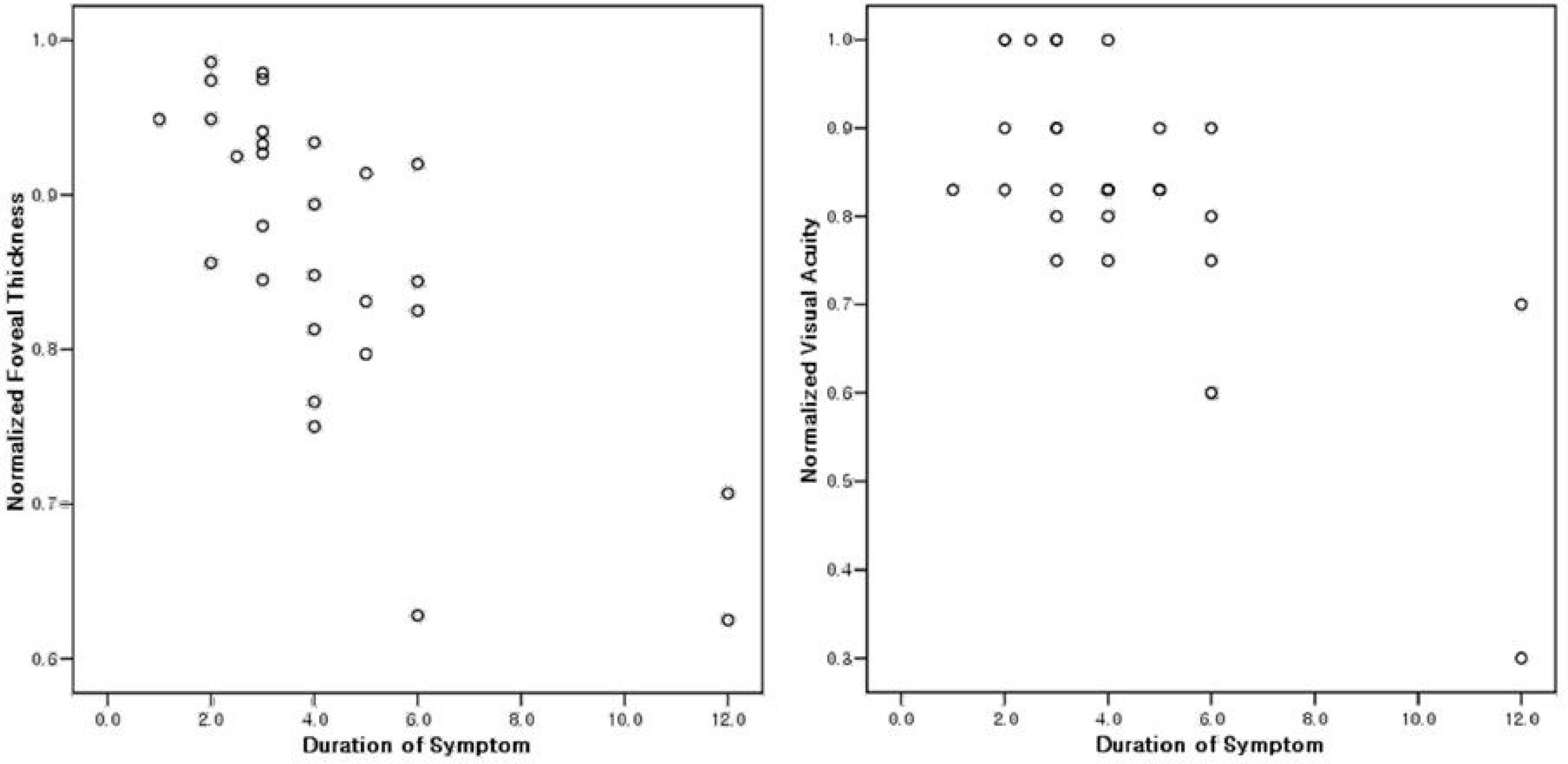
Figure 2. Relationship between normalized foveal thickness and duration of symptoms (left) and best-corrected visual acuity (BCVA) and duration of symptoms (right) in 28 patients with unilateral resolved central serous chorioretinopathy. Regression analysis demonstrated a significant decrease in relation to the duration of symptoms of both BCVA (r=-0.716, p<0.05, t-test) and foveal thickness (r=-0.736, p<0.05, two-sample /-test).
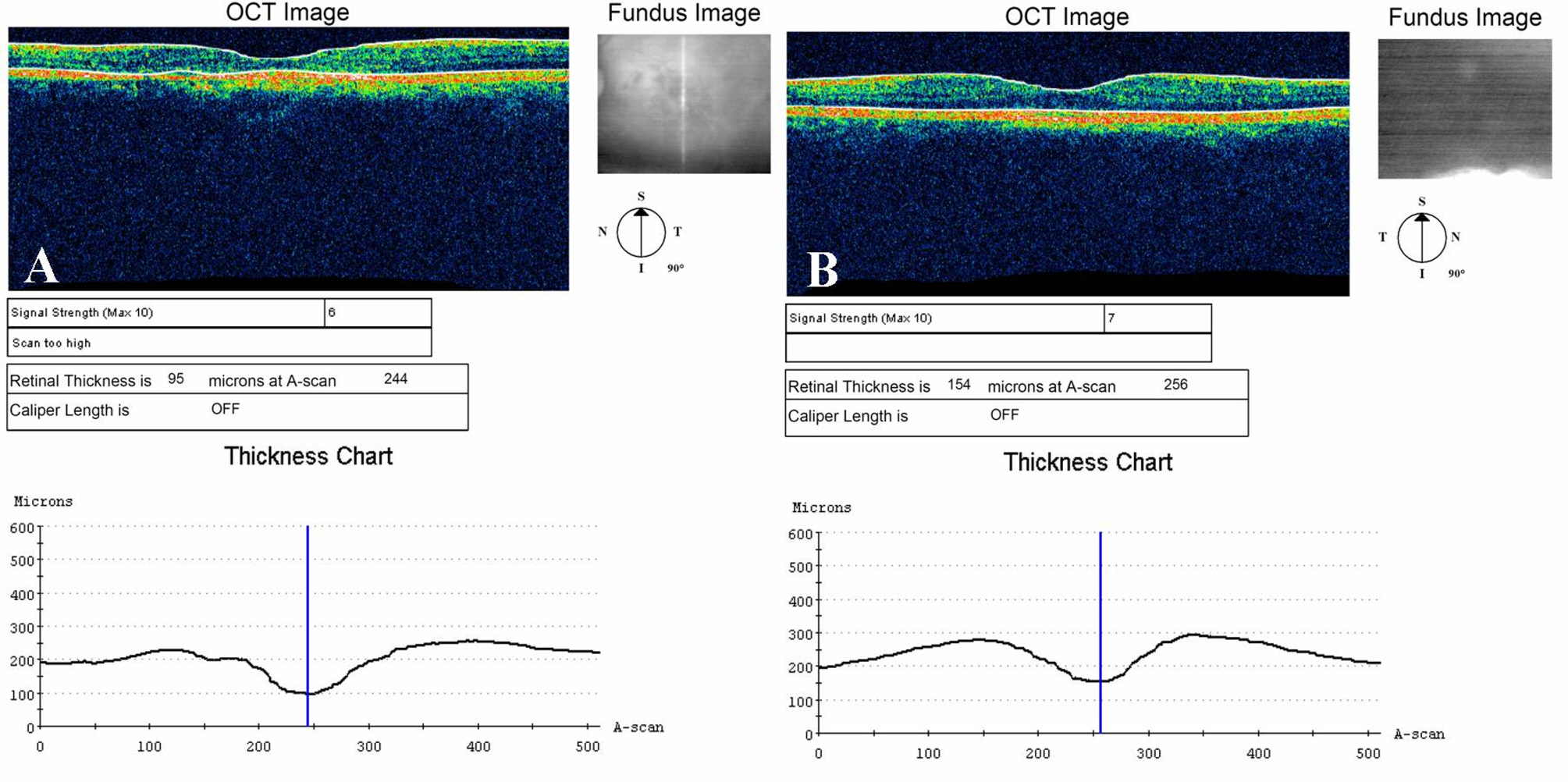
Figure 3. (A) OCT scan of the involved eye (visual acuity, 0.3), foveal thickness is attenuated (95 μm). (B) In the uninvolved eye (visual acuity, 1.0), foveal thickness is 154 μm. The normalized foveal thickness is 0.617 and the normalized visual acuity is 0.3.
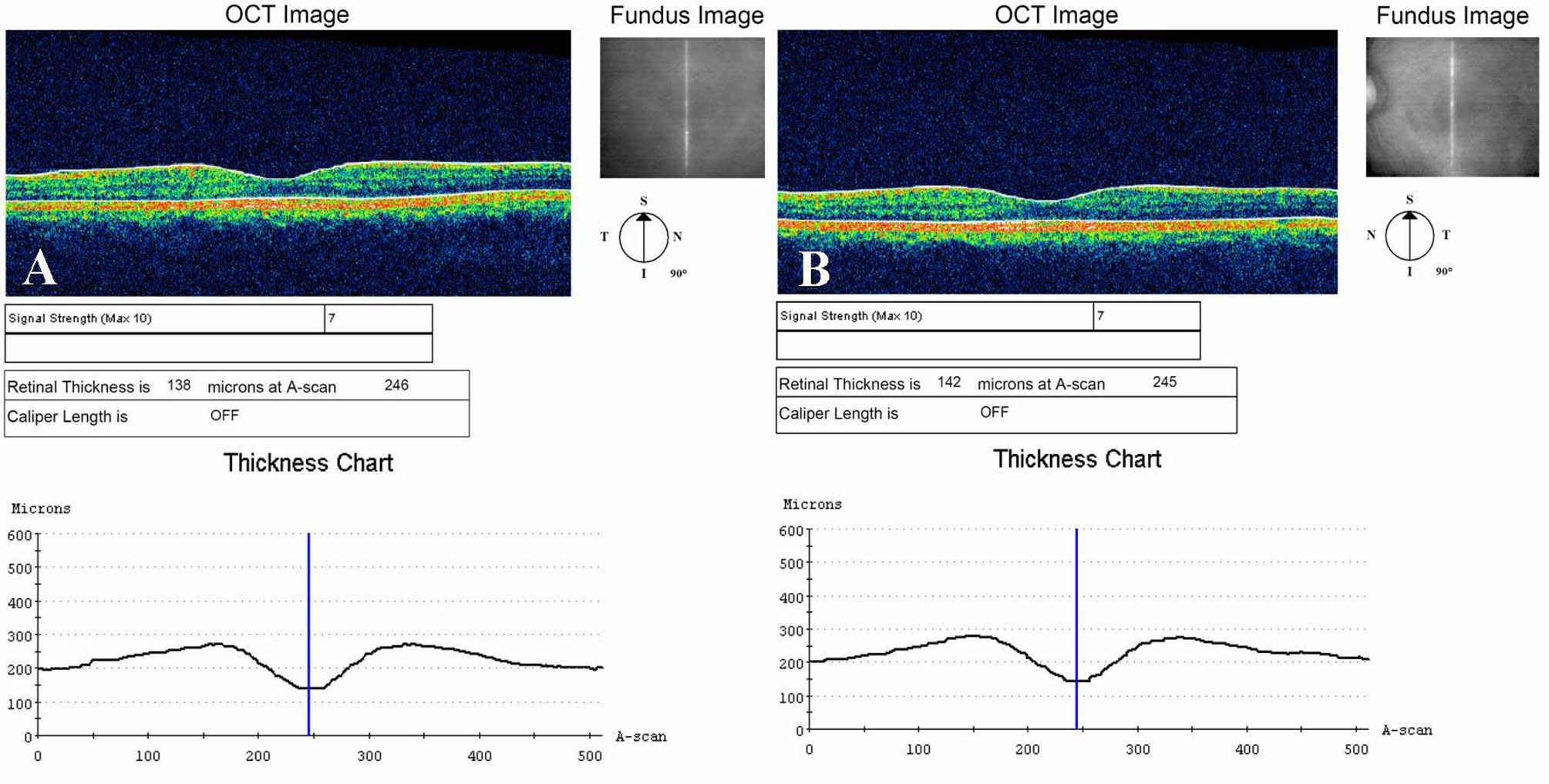
Figure 4. (A) The scan of the involved eye (visual acuity, 1.0). (B) The scan of the uninvolved eye. There is no difference between involved and uninvolved eye foveal thickness (138 μm, 142 μm). The normalized foveal thickness is 0.912, and the normalized visual acuity is 1.0.
Reference
-
References
1. Von Grafe A. Under centrale recidiverende retinitis. Arch Clin Exp Ophthalmol. 1866; 12:211–5.2. Ryan SJ. Retina. 2nd ed.St. Louis: SV Mosby;1994. p. 1158–68.3. Choi WH, Kim JW. The usefulness of OCT (Optical Cohrence Tomography) for the diagnosis of central serous chorioretinopathy. J Korean Ophthalmol Soc. 2000; 41:410–7.4. Habib MS, Cannon PS, Steel DH. The combination of intravitreal triamcinolone and phacoemulsification surgery in patients with diabetic foveal oedema and cataract. BMC Ophthalmol. 2005; 5:15.
Article5. Kim HK, Lee SC, Yun YS. The changes of sensory retinal detachment in central serous chorioretinal patients. J Korean Ophthalmol Soc. 2005; 46:71–7.6. Montero JA, Ruiz Moreno JM. Optical coherence tomography characterization of idiopathic central serous chorioretinopathy. Br J Ophthalmol. 2005; 89:562–4.7. Choi JH, Park JS. Quantitative measurement of neurosensory retinal detachment in central serous chorioretinopathy. J Korean Ophthalmol Soc. 1998; 39:1460–7.8. Chung CK, Chin HS, Moon YS. Comparision of results of electroretinogran, fluorescein angiogram and color vision test in acute central serous chorioretinopathy. J Korean Ophthalmol Soc. 2005; 46:71–7.9. Hee MR, Izatt JA, Swanson EA, et al. Optical coherence tomography of the human retina. Arch Ophthalmol. 1995; 113:325–32.
Article10. Huang D, Swanson EA, Lin CP, et al. Optical coherence tomography. Science. 1991; 254:1178–81.
Article11. Iida T, Yannuzzi LA, Spaide RF, et al. Cystoid macular degeneration in chronic central serous chorioretinopathy. Retina. 2003; 23:1–7.
Article12. Lee DY, Kim DH, Nam WH, et al. The optical coherence tomography analysis of hyperfluorescence by scanning laser ophthalmoscope in central serous chorioretinopahty. J Korean Ophthalmol Soc. 2005; 46:9961–68.13. Bujarborua D. Long term follow up of idiopathic central serous chorioteinopathy without laser. Acta Ophthalmol Scand. 2001; 79:417–21.14. Iida T, Hagimura N, Sato T, Kishi S. Evaluation of central serous chorioretinopathy with optical coherence tomography. Am J Ophthalmol. 2000; 129:16–20.
Article15. Klein ML, van Buskirk EM, Friedman E. Experience with nontreatment of central serous choriopathy. Arch Ophthalmol. 1974; 91:247–50.16. Jang HS, Shon OH, Kim HK. Clinical aspect of central serous chorioretinopathy. J Korean Ophthalmol Soc. 1988; 29:103–8.17. Baek HI, Yoon HM, Chi NC. Therapeutic result of laser photocoagulation for central serous chorioretinopathy. J Korean Ophthalmol Soc. 1990; 31:947–52.18. Kim SB, Chang HK. A Clinical Study of the more affected age group and over 50 years of age group in central serous chorioretinopathy characteristics. J Korean Ophthalmol Soc. 1994; 35:1217–25.19. Yoon KC, Seo MS, Lee MK, et al. Clinical anylsis of central serous chorioretinopathy. J Korean Ophthalmol Soc. 1998; 39:327–35.20. Eandi CM, Chung JE, Cardillo-Piccolino F, Spaide RF. Optical coherence tomography in unilateral resolved central serous chorioretinopathy. Retina. 2005; 25:417–21.
Article21. Wang MS, Sander B, Larsen M. Retinal atrophy in idiopathic central serous chorioretinopathy. Am J Ophthalmol. 2002; 133:787–93.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Photodynamic Therapy With Verteporfin using Half Fluence for Chronic Central Serous Chorioretinopathy
- Measurement and Analysis of Serous Fluid in Central Serous Chorioretinopathy using OCT
- Selective Retina Therapy in Patients with Central Serous Chorioretinopathy
- Photodynamic Therapy with Vertepofin for Short Time for Chronic Central Serous Chorioretinopathy
- A Case of Idiopathic Multiple Central Serous Chorioretinopathy
