Optimal Needle Placement for Extensor Hallucis Longus Muscle: A Cadaveric Study
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Korea University College of Medicine, Seoul, Korea. rmkdh@korea.ac.kr
- 2School of Kinesiology, University of British Columbia, Vancouver, Canada.
- KMID: 2327607
- DOI: http://doi.org/10.5535/arm.2016.40.3.457
Abstract
OBJECTIVE
To determine the midpoint (MD) of extensor hallucis longus muscle (EHL) and compare the accuracy of different needle electromyography (EMG) insertion techniques through cadaver dissection.
METHODS
Thirty-eight limbs of 19 cadavers were dissected. The MD of EHL was marked at the middle of the musculotendinous junction and proximal origin of EHL. Three different needle insertion points of EHL were marked following three different textbooks: M1, 3 fingerbreadths above bimalleolar line (BML); M2, junction between the middle and lower third of tibia; M3, 15 cm proximal to the lower border of both malleoli. The distance from BML to MD (BML_MD), and the difference between 3 different points (M1-3) and MD were measured (designated D1, D2, and D3, respectively). The lower leg length (LL) was measured from BML to top of medial condyle of tibia.
RESULTS
The median value of LL was 34.5 cm and BML_MD was 12.0 cm. The percentage of BML_MD to LL was 35.1%. D1, D2, and D3 were 7.0, 0.9, and 3.0 cm, respectively. D2 was the shortest, meaning needle placement following technique by Lee and DeLisa was closest to the actual midpoint of EHL.
CONCLUSION
The MD of EHL is approximately 12 cm above BML, and about distal 35% of lower leg length. Technique that recommends placing the needle at distal two-thirds of the lower leg (M2) is the most accurate method since the point was closest to muscle belly of EHL.
Figure
-
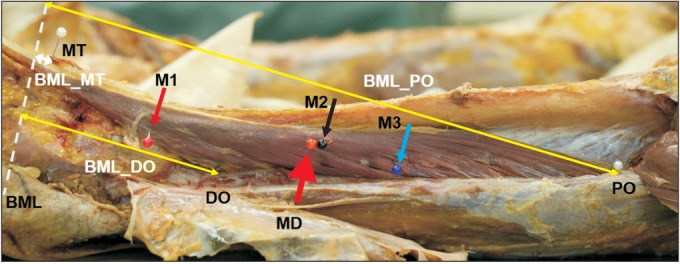
Fig. 1 Needle insertion sites according to three different commonly referred methods: M1, 3 fingerbreadths above the bimalleolar line; M2, junction between the middle and lower third of tibia; M3, 15 cm proximal to the lower border of both malleoli. Bimalleolar line was drawn between lower borders of both malleoli. The distance from bimalleolar line to proximal (BML_PO) and distal origin (BML_DO) of extensor hallucis longus (EHL) was calculated. Musculotendinous junction (MT) and midpoint (MD) of EHL was also marked.
Cited by 1 articles
-
Optimal Placement of Needle Electromyography in Extensor Indicis: A Cadaveric Study
Jin Young Im, Hong Bum Park, Seok Jun Lee, Seong Gyu Lim, Ki Hoon Kim, Dasom Kim, Im Joo Rhyu, Byung Kyu Park, Dong Hwee Kim
Ann Rehabil Med. 2018;42(3):473-476. doi: 10.5535/arm.2018.42.3.473.
Reference
-
1. Tezer M, Cicekcibasi AE. A variation of the extensor hallucis longus muscle (accessory extensor digiti secundus muscle). Anat Sci Int. 2012; 87:111–114. PMID: 21559883.
Article2. Gaber TA, Basu B, Shakespeare D, Singh R, Salam S, McFarlane J. Botulinum Toxin in the management of hitchhiker's toe. NeuroRehabilitation. 2011; 28:395–399. PMID: 21725174.
Article3. Vittoria N, Giuseppe M, Ivano D, Giovanni B. The innervation of extensor hallucis longus muscle: an anatomical study for selective neurotomy. Acta Neurochir (Wien). 2009; 151:1275–1279. PMID: 19730770.
Article4. Kim KH, Kim DH, Yun HS, Park BK, Jang JE. Optimal stimulation site for deep peroneal motor nerve conduction study around the ankle: cadaveric study. Ann Rehabil Med. 2012; 36:182–186. PMID: 22639741.
Article5. Berent S, Albers JW. Neurobehavioral toxicology: neurological and neuropsychological perspectives. London: Taylor & Francis;2005.6. Haig AJ, Goodmurphy CW, Harris AR, Ruiz AP, Etemad J. The accuracy of needle placement in lower-limb muscles: a blinded study. Arch Phys Med Rehabil. 2003; 84:877–882. PMID: 12808542.7. Perotto AO, Delagi EF, Iazzetti J, Morrison D. Anatomical guide for the electromyographer: the limbs and trunk. 4th ed. Springfield: Charles C Thomas Publisher;2005.8. Lee HJ, DeLisa JA. Manual of nerve conduction study and surface anatomy for needle electromyography. 4th ed. Philadelphia: Lippincott Williams & Wilkins;2005.9. Chu-Andrews J, Johnson RJ. Electrodiagnosis: an anatomical and clinical approach. Philadelphia: Lippincott;1986.10. Boon AJ, Oney-Marlow TM, Murthy NS, Harper CM, McNamara TR, Smith J. Accuracy of electromyography needle placement in cadavers: non-guided vs. ultrasound guided. Muscle Nerve. 2011; 44:45–49. PMID: 21674520.
Article11. Goodmurphy C, Chiodo A, Haig A. The accuracy of needle placement in extremity muscles: a blinded study. J Clin Neurophysiol. 2007; 24:366–378. PMID: 17938608.
Article12. Kurtis MM, Floyd AG, Yu QP, Pullman SL. High doses of botulinum toxin effectively treat disabling up-going toe. J Neurol Sci. 2008; 264:118–120. PMID: 17884097.
Article13. Sherman AL, Willick SP, Cardenas DD. Management of focal dystonia of the extensor hallucis longus muscle with botulinum toxin injection: a case report. Arch Phys Med Rehabil. 1998; 79:1303–1305. PMID: 9779689.
Article14. Elgafy H, Ebraheim NA, Shaheen PE, Yeasting RA. Extensor hallucis longus innervation: an anatomic study. Clin Orthop Relat Res. 2002; 398:245–251. PMID: 11964657.15. Dumitru D, Amato AA, Zwarts MJ. Electrodiagnostic medicine. 2nd ed. Philadelphia: Hanley & Belfus;2002.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Checkrein Deformity of Extensor Hallucis Longus Tendon and Extensor Retinaculum Syndrome with Deep Peroneal Nerve Entrapment after Triplane Fracture: A Case Report
- Reconstruction of Chronic Extensor Hallucis Longus Tendon Rupture Using Interposed Scar Tissue: A Case Report
- Anatomical Study of the Accessory Tendon of the Extensor Hallucis Longus Muscle and Its Clinical Application
- Complete Rupture of the Extensor Hallucis Longus Tendon with Accessory Slip Mimicking a Partial Rupture: A Case Report
- Split Transfer of Extensor Digitorum Longus of the Second Toe for Elongation of EHB after Modified Jones' Procedure
